

Safety and vaccine-induced HIV-1 immune responses in healthy volunteers following a late MVA-B boost 4 years after the last immunization
- PMID: 29065142
- PMCID: PMC5655491
- DOI: 10.1371/journal.pone.0186602
Safety and vaccine-induced HIV-1 immune responses in healthy volunteers following a late MVA-B boost 4 years after the last immunization
Erratum in
-
Correction: Safety and vaccine-induced HIV-1 immune responses in healthy volunteers following a late MVA-B boost 4 years after the last immunization.PLoS One. 2018 Apr 10;13(4):e0195915. doi: 10.1371/journal.pone.0195915. eCollection 2018. PLoS One. 2018. PMID: 29634751 Free PMC article.
Abstract
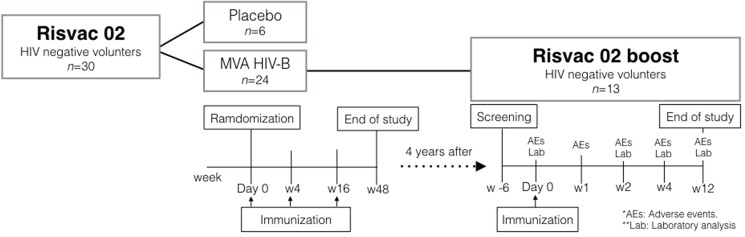
Background: We have previously shown that an HIV vaccine regimen including three doses of HIV-modified vaccinia virus Ankara vector expressing HIV-1 antigens from clade B (MVA-B) was safe and elicited moderate and durable (1 year) T-cell and antibody responses in 75% and 95% of HIV-negative volunteers (n = 24), respectively (RISVAC02 study). Here, we describe the long-term durability of vaccine-induced responses and the safety and immunogenicity of an additional MVA-B boost.
Methods: 13 volunteers from the RISVAC02 trial were recruited to receive a fourth dose of MVA-B 4 years after the last immunization. End-points were safety, cellular and humoral immune responses to HIV-1 and vector antigens assessed by ELISPOT, intracellular cytokine staining (ICS) and ELISA performed before and 2, 4 and 12 weeks after receiving the boost.
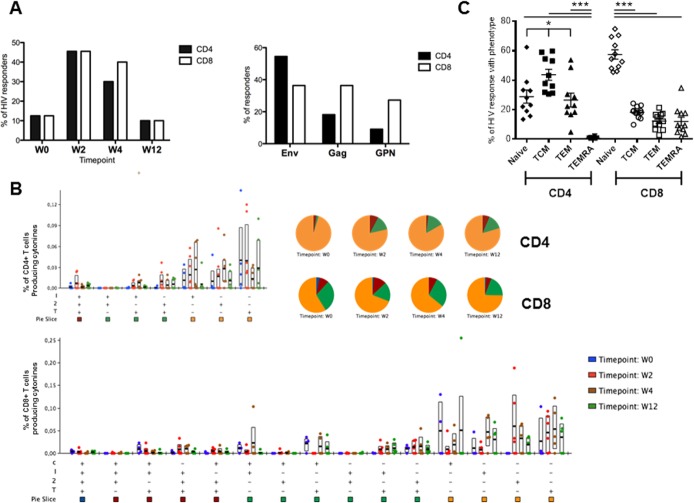
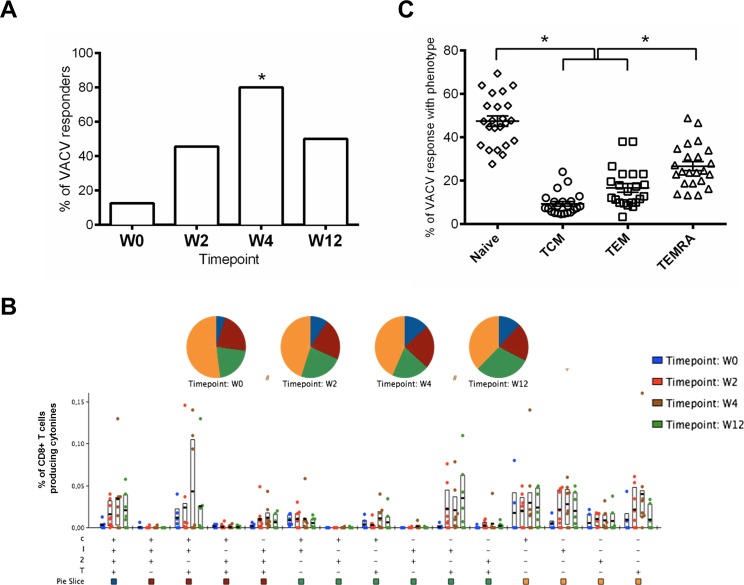
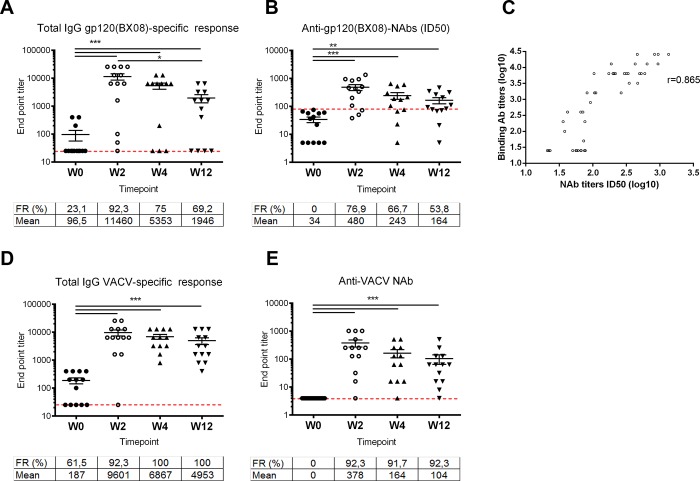
Results: Volunteers reported 64 adverse events (AEs), although none was a vaccine-related serious AE. After 4 years from the 1st dose of the vaccine, only 2 volunteers maintained low HIV-specific T-cell responses. After the late MVA-B boost, a modest increase in IFN-γ T-cell responses, mainly directed against Env, was detected by ELISPOT in 5/13 (38%) volunteers. ICS confirmed similar results with 45% of volunteers showing that CD4+ T-cell responses were mainly directed against Env, whereas CD8+ T cell-responses were similarly distributed against Env, Gag and GPN. In terms of antibody responses, 23.1% of the vaccinees had detectable Env-specific binding antibodies 4 years after the last MVA-B immunization with a mean titer of 96.5. The late MVA-B boost significantly improved both the response rate (92.3%) and the magnitude of the systemic binding antibodies to gp120 (mean titer of 11460). HIV-1 neutralizing antibodies were also enhanced and detected in 77% of volunteers. Moreover, MVA vector-specific T cell and antibody responses were boosted in 80% and 100% of volunteers respectively.
Conclusions: One boost of MVA-B four years after receiving 3 doses of the same vaccine was safe, induced moderate increases in HIV-specific T cell responses in 38% of volunteers but significantly boosted the binding and neutralizing antibody responses to HIV-1 and to the MVA vector.
Trial registration: ClinicalTrials.gov NCT01923610.
Conflict of interest statement
Figures

References
-
- Rerks-Ngarm S, Pitisuttithum P, Nitayaphan S, Kaewkungwal J, Chiu J, Paris R, et al. Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N Engl J Med 2009; 361(23):2209–2220. doi: 10.1056/NEJMoa0908492 - DOI - PubMed
-
- Antoine G, Scheiflinger F, Dorner F, Falkner FG. The complete genomic sequence of the modified vaccinia Ankara strain: comparison with other orthopoxviruses. Virology 1998; 244(2):365–396. doi: 10.1006/viro.1998.9123 - DOI - PubMed
-
- Pantaleo G, Esteban M, Jacobs B, Tartaglia J. Poxvirus vector-based HIV vaccines. Curr Opin HIV AIDS 2010; 5(5):391–396. doi: 10.1097/COH.0b013e32833d1e87 - DOI - PubMed
-
- Gomez CE, Perdiguero B, Garcia-Arriaza J, Esteban M. Poxvirus vectors as HIV/AIDS vaccines in humans. Hum Vaccin Immunother 2012; 8(9):1192–1207. doi: 10.4161/hv.20778 - DOI - PMC - PubMed
-
- Sanchez-Sampedro L, Perdiguero B, Mejias-Perez E, Garcia-Arriaza J, Di PM, Esteban M. The evolution of poxvirus vaccines. Viruses 2015; 7(4):1726–1803. doi: 10.3390/v7041726 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
