

Clinical Course of Sarcoidosis in World Trade Center-Exposed Firefighters
- PMID: 29066387
- PMCID: PMC6026251
- DOI: 10.1016/j.chest.2017.10.014
Clinical Course of Sarcoidosis in World Trade Center-Exposed Firefighters
Abstract
Background: Sarcoidosis is believed to represent a genetically primed, abnormal immune response to an antigen exposure or inflammatory trigger, with both genetic and environmental factors playing a role in disease onset and phenotypic expression. In a population of firefighters with post-World Trade Center (WTC) 9/11/2001 (9/11) sarcoidosis, we have a unique opportunity to describe the clinical course of incident sarcoidosis during the 15 years postexposure and, on average, 8 years following diagnosis.
Methods: Among the WTC-exposed cohort, 74 firefighters with post-9/11 sarcoidosis were identified through medical records review. A total of 59 were enrolled in follow-up studies. For each participant, the World Association of Sarcoidosis and Other Granulomatous Diseases organ assessment tool was used to categorize the sarcoidosis involvement of each organ system at time of diagnosis and at follow-up.
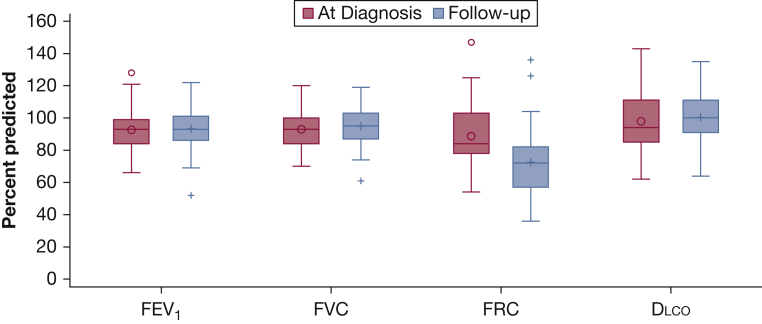
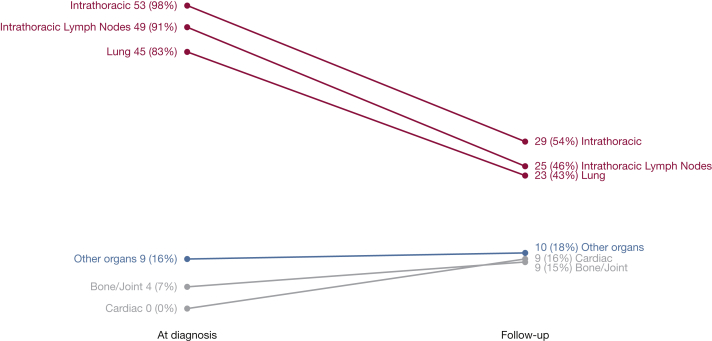
Results: The incidence of sarcoidosis post-9/11 was 25 per 100,000. Radiographic resolution of intrathoracic involvement occurred in 24 (45%) subjects. Lung function for nearly all subjects was within normal limits. Extrathoracic involvement increased, most prominently joints (15%) and cardiac (16%) involvement. There was no evidence of calcium dysmetabolism. Few subjects had ocular (5%) or skin (2%) involvement, and none had beryllium sensitization. Most (76%) subjects did not receive any treatment.
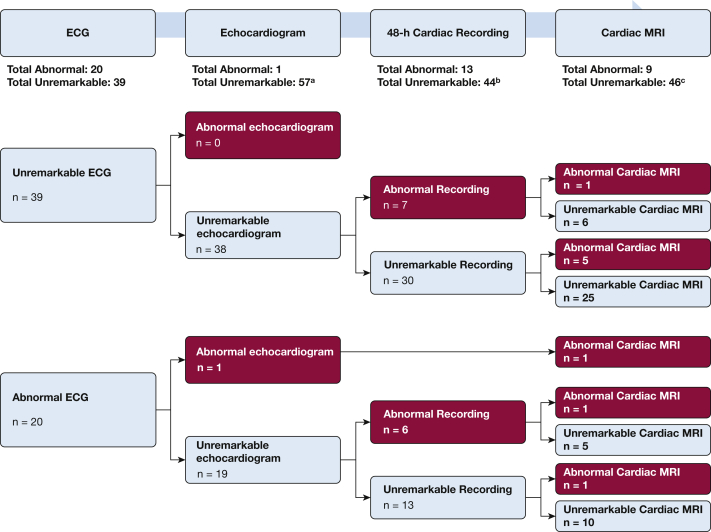
Conclusions: Extrathoracic disease was more prevalent in WTC-related sarcoidosis than reported for patients with sarcoidosis without WTC exposure or for other exposure-related granulomatous diseases (beryllium disease and hypersensitivity pneumonitis). Cardiac involvement would have been missed if evaluation stopped after ECG, 48-h recordings, and echocardiogram. Our results also support the need for advanced cardiac screening in asymptomatic patients with strenuous, stressful, public safety occupations, given the potential fatality of a missed diagnosis.
Keywords: World Trade Center; clinical course; firefighters; sarcoidosis.
Copyright © 2017 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Sarcoidosis in World Trade Center-Exposed Firefighters.Chest. 2018 Apr;153(4):1072-1073. doi: 10.1016/j.chest.2017.11.045. Chest. 2018. PMID: 29626952 No abstract available.
References
-
- Valeyre D., Prasse A., Nunes H., Uzunhan Y., Brillet P.Y., Muller-Quernheim J. Sarcoidosis. Lancet. 2014;383(9923):1155–1167. - PubMed
-
- Iannuzzi M.C., Rybicki B.A., Teirstein A.S. Sarcoidosis. N Engl J Med. 2007;357(21):2153–2165. - PubMed
-
- O'Regan A., Berman J.S. Sarcoidosis. Ann Intern Med. 2012;156(9) ITC5-1, ITC5-2, ITC5-3, ITC5-4, ITC5-5, ITC5-6, ITC5-7, ITC5-8, ITC5-9, ITC5-10, ITC15-11, ITC15-12, ITC15-13, ITC15-14, ITC15-15; quiz ITC15-16. - PubMed
-
- Rybicki B.A., Major M., Popovich J., Jr., Maliarik M.J., Iannuzzi M.C. Racial differences in sarcoidosis incidence: a 5-year study in a health maintenance organization. Am J Epidemiol. 1997;145(3):234–241. - PubMed
-
- Rybicki B.A., Maliarik M.J., Major M., Popovich J., Jr., Iannuzzi M.C. Epidemiology, demographics, and genetics of sarcoidosis. Semin Respir Infect. 1998;13(3):166–173. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
