

Interleukin-6 and the Risk of Adverse Outcomes in Patients After an Acute Coronary Syndrome: Observations From the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52) Trial
- PMID: 29066436
- PMCID: PMC5721825
- DOI: 10.1161/JAHA.117.005637
Interleukin-6 and the Risk of Adverse Outcomes in Patients After an Acute Coronary Syndrome: Observations From the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52) Trial
Abstract
Background: Interleukin-6 (IL-6) is an inflammatory cytokine implicated in plaque instability in acute coronary syndrome (ACS). We aimed to evaluate the prognostic implications of IL-6 post-ACS.
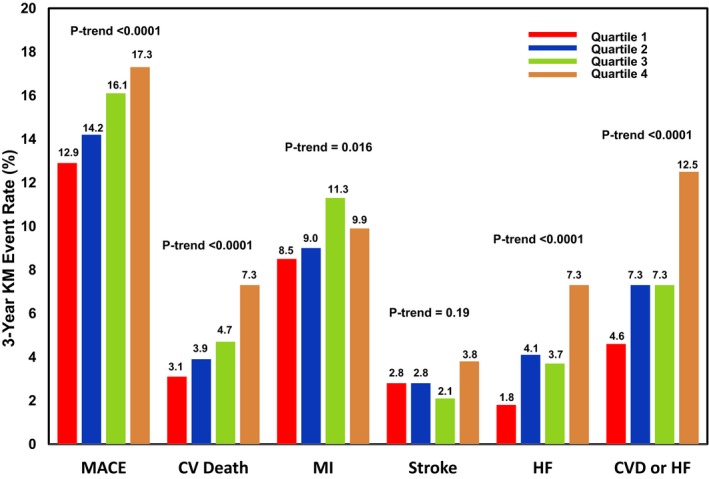
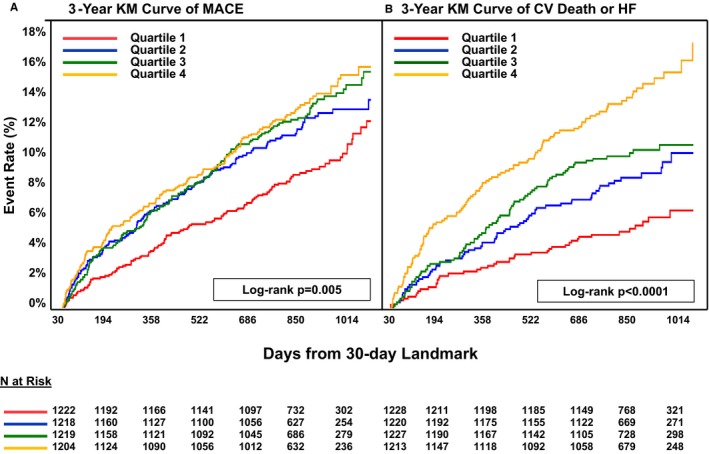
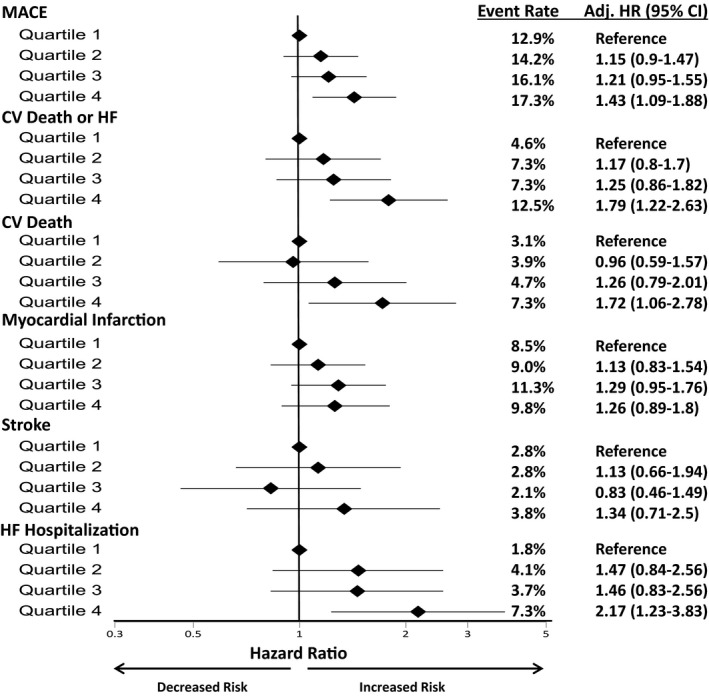
Methods and results: IL-6 concentration was assessed at baseline in 4939 subjects in SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52), a randomized trial of darapladib in patients ≤30 days from ACS. Patients were followed for a median of 2.5 years for major adverse cardiovascular events; cardiovascular death, myocardial infarction, or stroke) and cardiovascular death or heart failure hospitalization. Primary analyses were adjusted first for baseline characteristics, days from index ACS, ACS type, and randomized treatment arm. For every SD increase in IL-6, there was a 10% higher risk of major adverse cardiovascular events (adjusted hazard ratio [adj HR] 1.10, 95% confidence interval [CI] 1.01-1.19) and a 22% higher risk of cardiovascular death or heart failure (adj HR 1.22, 95% CI 1.11-1.34). Patients in the highest IL-6 quartile had a higher risk of major adverse cardiovascular events (adj HR Q4:Q1 1.57, 95% CI 1.22-2.03) and cardiovascular death or heart failure (adj HR 2.29, 95% CI 1.6-3.29). After further adjustment for biomarkers (high-sensitivity C-reactive protein, lipoprotein-associated phospholipase A2 activity, high-sensitivity troponin I, and B-type natriuretic peptide), IL-6 remained significantly associated with the risk of major adverse cardiovascular events (adj HR Q4:Q1 1.43, 95% CI 1.09-1.88) and cardiovascular death or heart failure (adj HR 1.79, 95% CI 1.22-2.63).
Conclusions: In patients after ACS, IL-6 concentration is associated with adverse cardiovascular outcomes independent of established risk predictors and biomarkers. These findings lend support to the concept of IL-6 as a potential therapeutic target in patients with unstable ischemic heart disease.
Keywords: acute coronary syndrome; atherosclerosis; biomarker; inflammation; vascular biology.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Pretenders and Contenders: Inflammation, C-Reactive Protein, and Interleukin-6.J Am Heart Assoc. 2017 Oct 24;6(10):e007490. doi: 10.1161/JAHA.117.007490. J Am Heart Assoc. 2017. PMID: 29066450 Free PMC article. No abstract available.
References
-
- Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473:317–325. - PubMed
-
- Yudkin JS, Kumari M, Humphries SE, Mohamed‐Ali V. Inflammation, obesity, stress and coronary heart disease: is interleukin‐6 the link? Atherosclerosis. 2000;148:209–214. - PubMed
-
- Schieffer B, Selle T, Hilfiker A, Hilfiker‐Kleiner D, Grote K, Tietge UJ, Trautwein C, Luchtefeld M, Schmittkamp C, Heeneman S, Daemen MJ, Drexler H. Impact of interleukin‐6 on plaque development and morphology in experimental atherosclerosis. Circulation. 2004;110:3493–3500. - PubMed
-
- Ridker PM, Rifai N, Stampfer M, Hennekens C. Plasma concentration of interleukin‐6 and the risk of future myocardial infarction among apparently healthy men. Circulation. 2000;101:1767–1772. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
