

Inflammatory Biomarkers Interleukin-6 and C-Reactive Protein and Outcomes in Stable Coronary Heart Disease: Experiences From the STABILITY (Stabilization of Atherosclerotic Plaque by Initiation of Darapladib Therapy) Trial
- PMID: 29066452
- PMCID: PMC5721818
- DOI: 10.1161/JAHA.116.005077
Inflammatory Biomarkers Interleukin-6 and C-Reactive Protein and Outcomes in Stable Coronary Heart Disease: Experiences From the STABILITY (Stabilization of Atherosclerotic Plaque by Initiation of Darapladib Therapy) Trial
Abstract
Background: Evaluation of cardiovascular prognosis in patients with stable coronary heart disease is based on clinical characteristics and biomarkers indicating dysglycemia, dyslipidemia, renal dysfunction, and possibly cardiac dysfunction. Inflammation plays a key role in atherosclerosis, but the association between inflammatory biomarkers and clinical outcomes is less studied in this population.
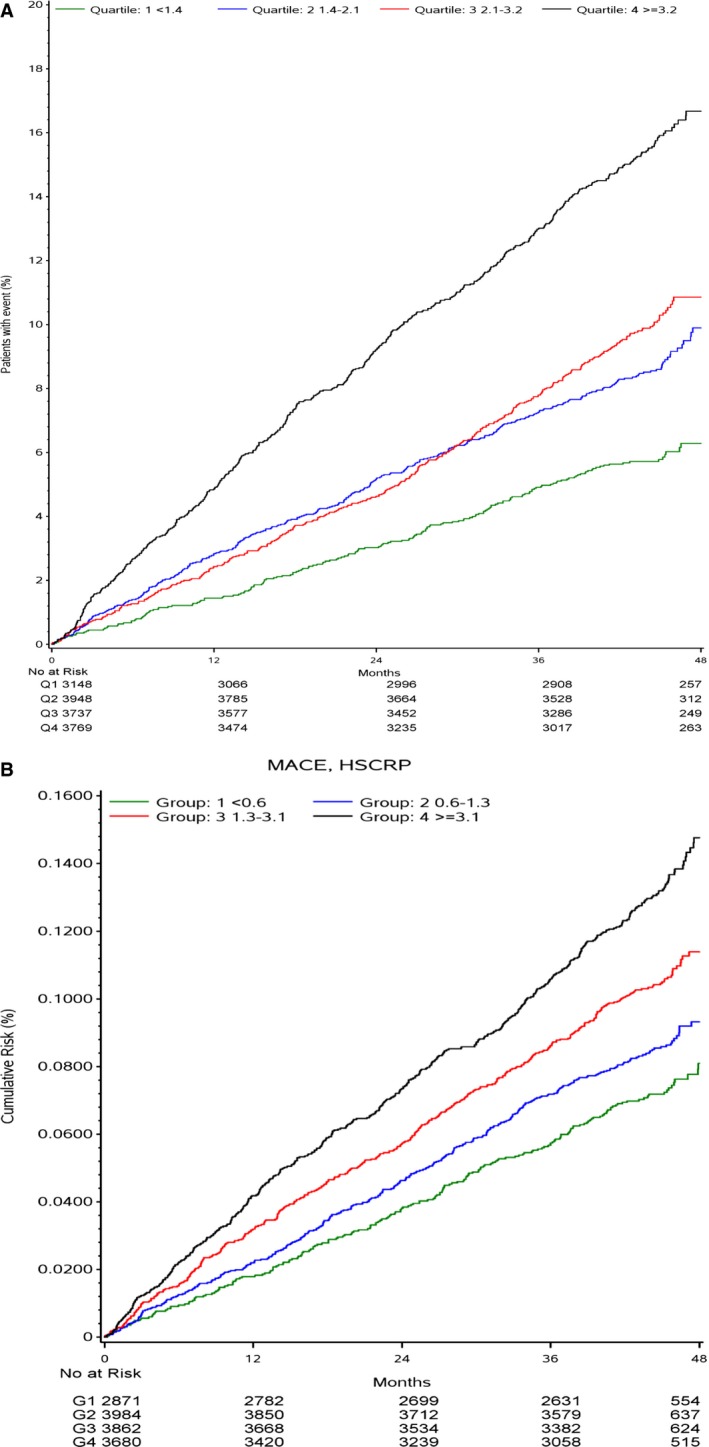
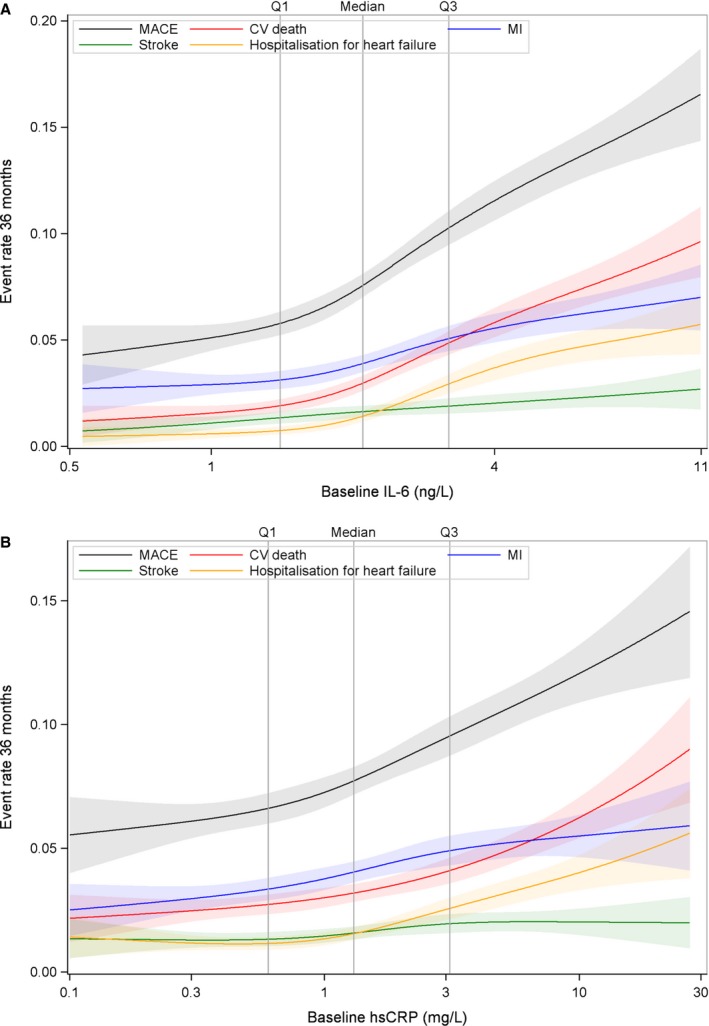
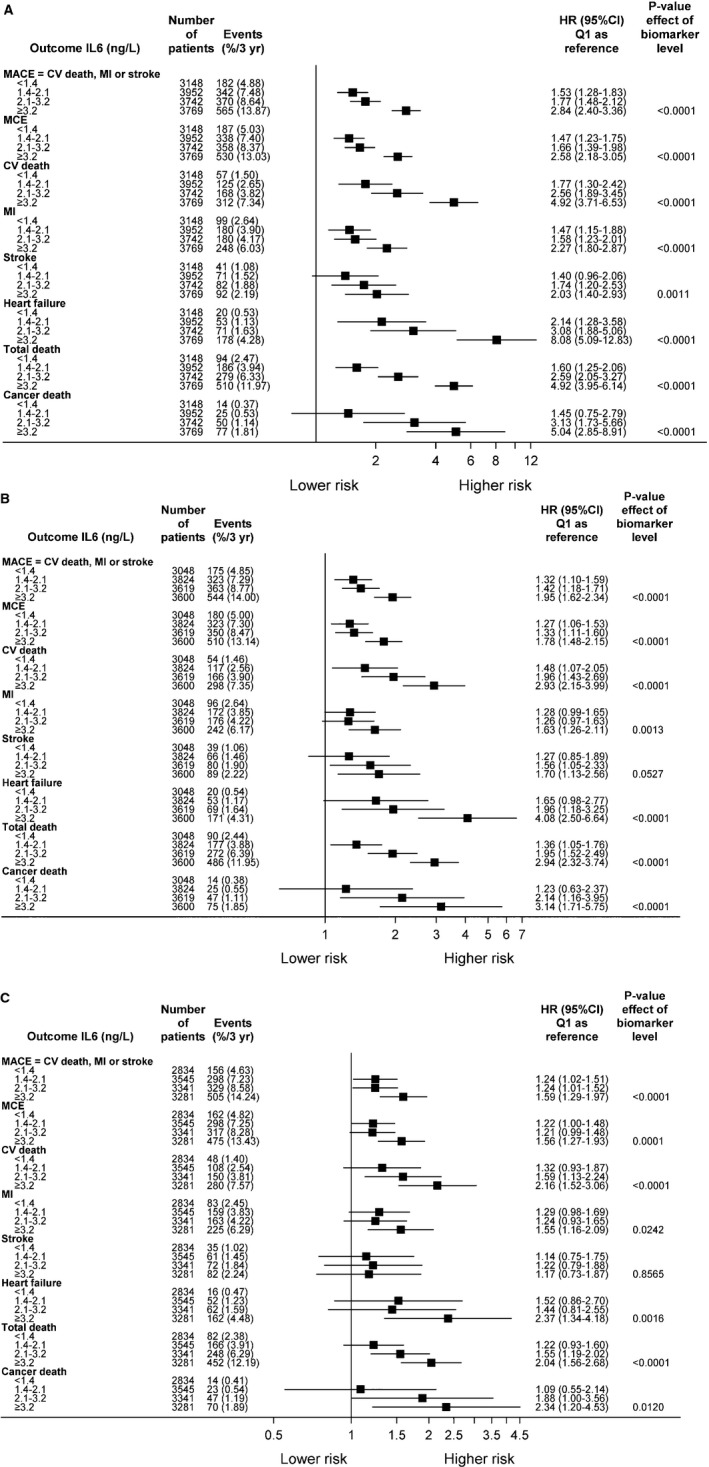
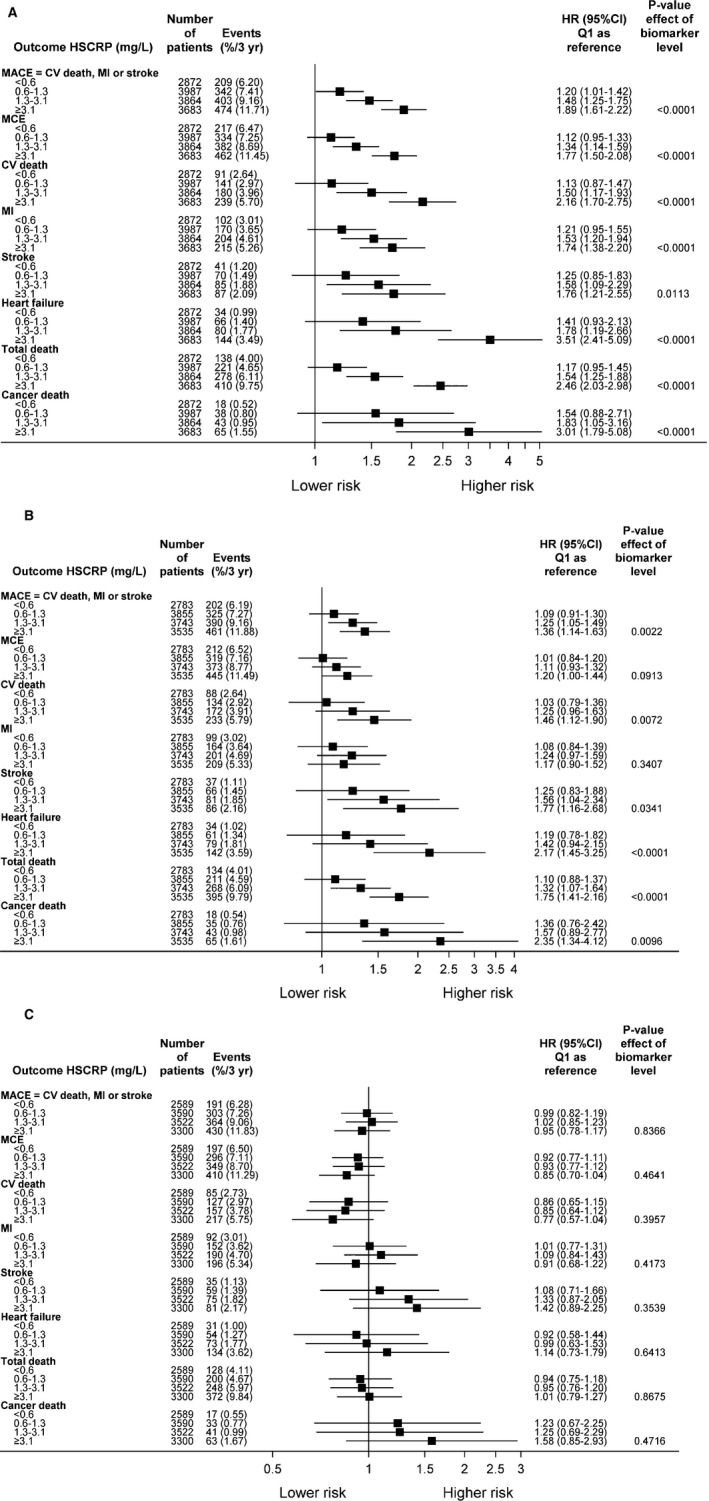
Methods and results: Overall, 15 828 patients with coronary heart disease in the STABILITY (Stabilization of Atherosclerotic Plaque by Initiation of Darapladib Therapy) trial were randomized to treatment with darapladib or placebo and observed for a median of 3.7 years. In 14 611 patients, levels of interleukin-6 (IL-6) and high-sensitivity C-reactive protein were measured in plasma samples: median levels were 2.1 (interquartile range, 1.4-3.2) ng/L and 1.3 (interquartile range, 0.6-3.1) mg/L, respectively. Associations between continuous levels or quartile groups and adjudicated outcomes were evaluated by spline graphs and Cox regression adjusted for clinical factors and cardiovascular biomarkers. IL-6 was associated with increased risk of major adverse cardiovascular events (quartile 4 versus quartile 1 hazard ratio [HR], 1.60; 95% confidence interval [CI], 1.30-1.97; P<0.0001); cardiovascular death (HR, 2.15; 95% CI, 1.53-3.04; P<0.0001); myocardial infarction (HR, 1.53; 95% CI, 1.14-2.04; P<0.05); all-cause mortality (HR, 2.11; 95% CI, 1.62-2.76; P<0.0001); and risk of hospitalization for heart failure (HR, 2.28; 95% CI, 1.34-3.89; P<0.001). Cancer death was doubled in the highest IL-6 quartile group (HR, 2.34; 95% CI, 1.20-4.53; P<0.05). High-sensitivity C-reactive protein was associated with both cardiovascular and non-cardiovascular events in the unadjusted model, but these did not remain after multivariable adjustments.
Conclusions: IL-6, an upstream inflammatory marker, was independently associated with the risk of major adverse cardiovascular events, cardiovascular and all-cause mortality, myocardial infarction, heart failure, and cancer mortality in patients with stable coronary heart disease. IL-6 might reflect a pathophysiological process involved in the development of these events.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00799903.
Keywords: C‐reactive protein; coronary disease; inflammation; interleukin‐6; white blood cells.
© 2017 The Authors and GlaxoSmithKline. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Pretenders and Contenders: Inflammation, C-Reactive Protein, and Interleukin-6.J Am Heart Assoc. 2017 Oct 24;6(10):e007490. doi: 10.1161/JAHA.117.007490. J Am Heart Assoc. 2017. PMID: 29066450 Free PMC article. No abstract available.
References
-
- Hartman J, Frishman WH. Inflammation and atherosclerosis: a review of the role of interleukin‐6 in the development of atherosclerosis and the potential for targeted drug therapy. Cardiol Rev. 2014;22:147–151. - PubMed
-
- Danesh J, Wheeler JG, Hirschfield GM, Eda S, Eiriksdottir G, Rumley A, Lowe GD, Pepys MB, Gudnason V. C‐reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med. 2004;350:1387–1397. - PubMed
-
- Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med. 1997;336:973–979. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
