

Association of Prehospital Blood Product Transfusion During Medical Evacuation of Combat Casualties in Afghanistan With Acute and 30-Day Survival
- PMID: 29067429
- PMCID: PMC5818807
- DOI: 10.1001/jama.2017.15097
Association of Prehospital Blood Product Transfusion During Medical Evacuation of Combat Casualties in Afghanistan With Acute and 30-Day Survival
Abstract
Importance: Prehospital blood product transfusion in trauma care remains controversial due to poor-quality evidence and cost. Sequential expansion of blood transfusion capability after 2012 to deployed military medical evacuation (MEDEVAC) units enabled a concurrent cohort study to focus on the timing as well as the location of the initial transfusion.
Objective: To examine the association of prehospital transfusion and time to initial transfusion with injury survival.
Design, setting, and participants: Retrospective cohort study of US military combat casualties in Afghanistan between April 1, 2012, and August 7, 2015. Eligible patients were rescued alive by MEDEVAC from point of injury with either (1) a traumatic limb amputation at or above the knee or elbow or (2) shock defined as a systolic blood pressure of less than 90 mm Hg or a heart rate greater than 120 beats per minute.
Exposures: Initiation of prehospital transfusion and time from MEDEVAC rescue to first transfusion, regardless of location (ie, prior to or during hospitalization). Transfusion recipients were compared with nonrecipients (unexposed) for whom transfusion was delayed or not given.
Main outcomes and measures: Mortality at 24 hours and 30 days after MEDEVAC rescue were coprimary outcomes. To balance injury severity, nonrecipients of prehospital transfusion were frequency matched to recipients by mechanism of injury, prehospital shock, severity of limb amputation, head injury, and torso hemorrhage. Cox regression was stratified by matched groups and also adjusted for age, injury year, transport team, tourniquet use, and time to MEDEVAC rescue.
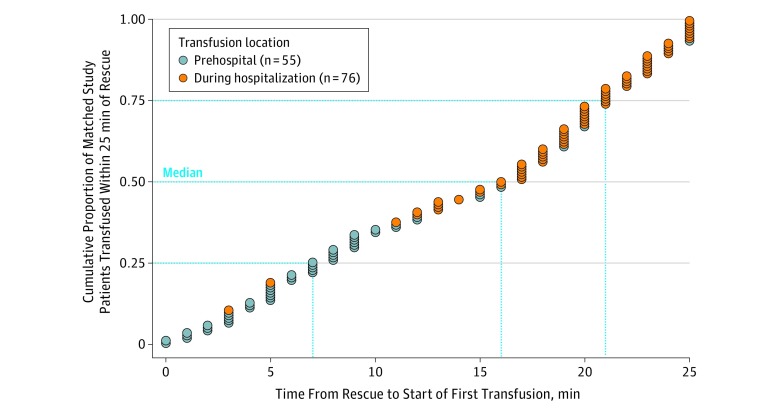
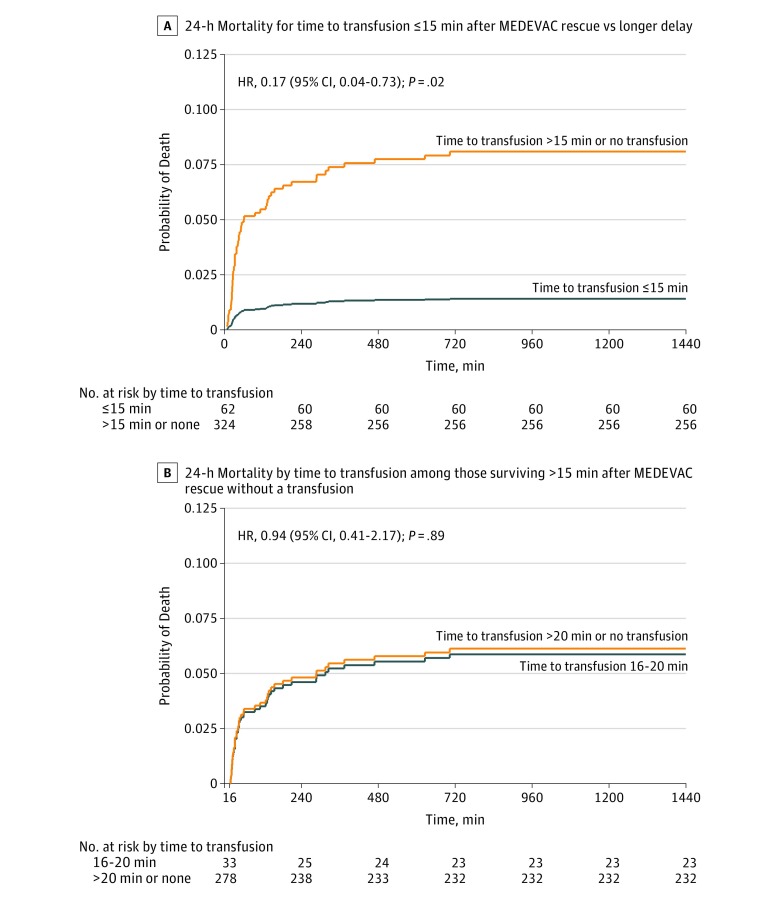
Results: Of 502 patients (median age, 25 years [interquartile range, 22 to 29 years]; 98% male), 3 of 55 prehospital transfusion recipients (5%) and 85 of 447 nonrecipients (19%) died within 24 hours of MEDEVAC rescue (between-group difference, -14% [95% CI, -21% to -6%]; P = .01). By day 30, 6 recipients (11%) and 102 nonrecipients (23%) died (between-group difference, -12% [95% CI, -21% to -2%]; P = .04). For the 386 patients without missing covariate data among the 400 patients within the matched groups, the adjusted hazard ratio for mortality associated with prehospital transfusion was 0.26 (95% CI, 0.08 to 0.84, P = .02) over 24 hours (3 deaths among 54 recipients vs 67 deaths among 332 matched nonrecipients) and 0.39 (95% CI, 0.16 to 0.92, P = .03) over 30 days (6 vs 76 deaths, respectively). Time to initial transfusion, regardless of location (prehospital or during hospitalization), was associated with reduced 24-hour mortality only up to 15 minutes after MEDEVAC rescue (median, 36 minutes after injury; adjusted hazard ratio, 0.17 [95% CI, 0.04 to 0.73], P = .02; there were 2 deaths among 62 recipients vs 68 deaths among 324 delayed transfusion recipients or nonrecipients).
Conclusions and relevance: Among medically evacuated US military combat causalities in Afghanistan, blood product transfusion prehospital or within minutes of injury was associated with greater 24-hour and 30-day survival than delayed transfusion or no transfusion. The findings support prehospital transfusion in this setting.
Conflict of interest statement
Figures


Comment in
-
Prehospital Blood Transfusion for Combat Casualties.JAMA. 2017 Oct 24;318(16):1548-1549. doi: 10.1001/jama.2017.15096. JAMA. 2017. PMID: 29067405 No abstract available.
-
Prehospital Blood Product Transfusion and Combat Injury Survival.JAMA. 2018 Mar 20;319(11):1166-1167. doi: 10.1001/jama.2017.21676. JAMA. 2018. PMID: 29558545 No abstract available.
References
-
- Eastridge BJ, Mabry RL, Seguin P, et al. Death on the battlefield (2001-2011): implications for the future of combat casualty care [published correction appears in J Trauma Acute Care Surg. 2013;74(2):706]. J Trauma Acute Care Surg. 2012;73(6)(suppl 5):S431-S437. - PubMed
-
- Davis JS, Satahoo SS, Butler FK, et al. An analysis of prehospital deaths: who can we save? J Trauma Acute Care Surg. 2014;77(2):213-218. - PubMed
-
- National Academies of Sciences, Engineering, and Medicine A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths after Injury. Washington, DC: National Academies Press; 2016. - PubMed
-
- Kragh JF Jr, Walters TJ, Baer DG, et al. Survival with emergency tourniquet use to stop bleeding in major limb trauma. Ann Surg. 2009;249(1):1-7. - PubMed
-
- Kotwal RS, Howard JT, Orman JA, et al. The effect of a golden hour policy on the morbidity and mortality of combat casualties. JAMA Surg. 2016;151(1):15-24. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
