

Atypical hemolytic uremic syndrome induced by CblC subtype of methylmalonic academia: A case report and literature review
- PMID: 29068997
- PMCID: PMC5671830
- DOI: 10.1097/MD.0000000000008284
Atypical hemolytic uremic syndrome induced by CblC subtype of methylmalonic academia: A case report and literature review
Abstract
Rationale: Methylmalonic acidemia (MMA) is a common organic acidemia, mainly due to methylmalonyl-CoA mutase (MCM) or its coenzyme cobalamin (VitB12) metabolic disorders. Cobalamin C (CblC) type is the most frequent inborn error of cobalamin metabolism; it can develop symptoms in childhood and often combine multisystem damage, which leads to methylmalonic acid, propionic acid, methyl citrate, and other metabolites abnormal accumulation, causing nerve, liver, kidney, bone marrow, and other organ damage.
Patient concerns: A 4-year-old girl presented with paleness, fatigue, severe normochromic anemia, and acute kidney injury.
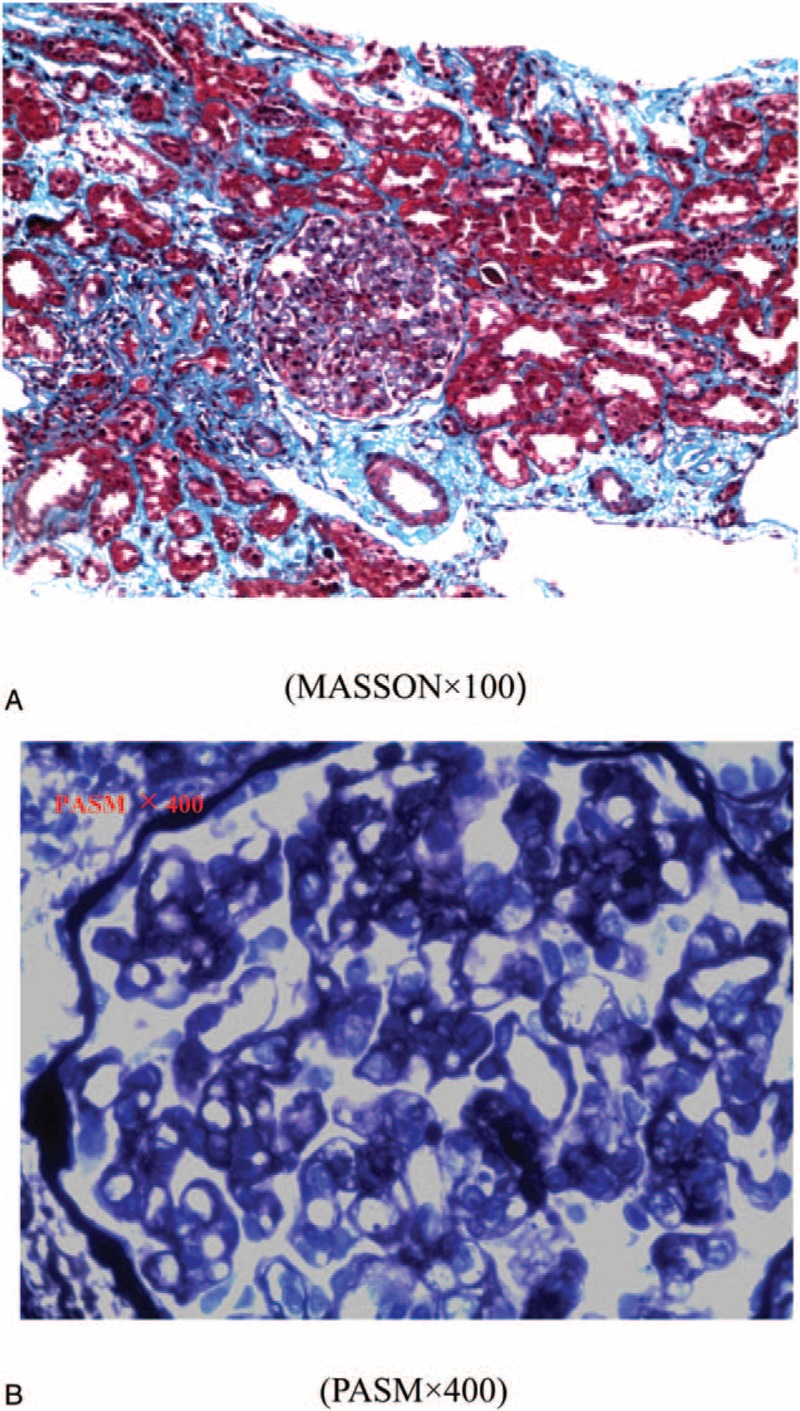
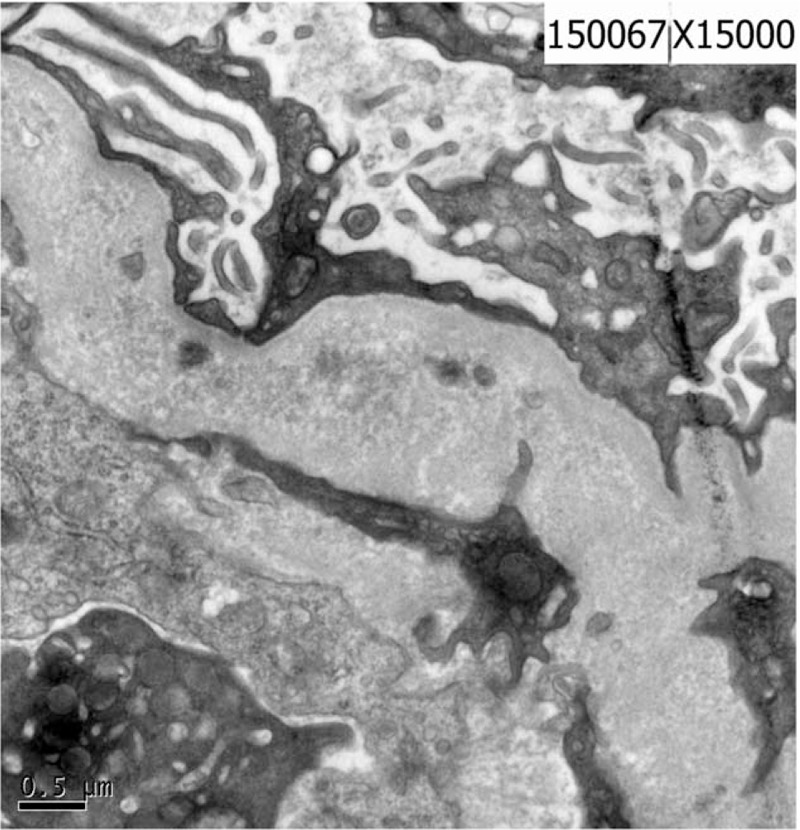
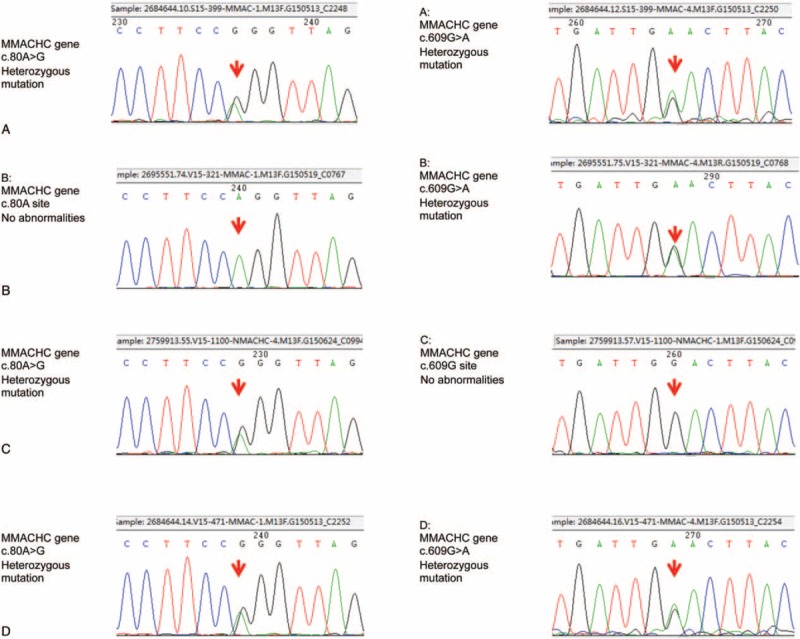
Diagnosis: Based on severe normochromic anemia and acute kidney injury, renal biopsy showed membranous proliferative glomerular lesions and thrombotic microvascular disease, supporting the diagnosis of aHUS. Although the serum vitamin B12 was normal, further investigation found the concentration of urinary methylmalonic acid and serum homocysteine increased obviously, genetic analysis revealed a heterozygous MMACHC mutation (exonl: c. 80A >G, c. 609G >A). The final diagnosis was aHUS induced by inherited methylmalonic acidemia (MMACHC heterozygous mutation exonl: c. 80A >G, c. 609G >A).
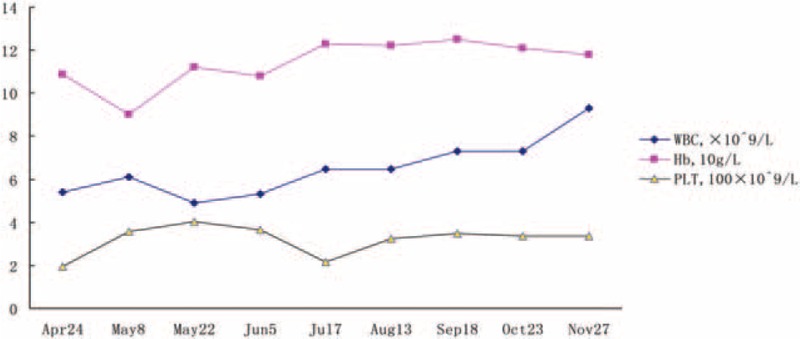
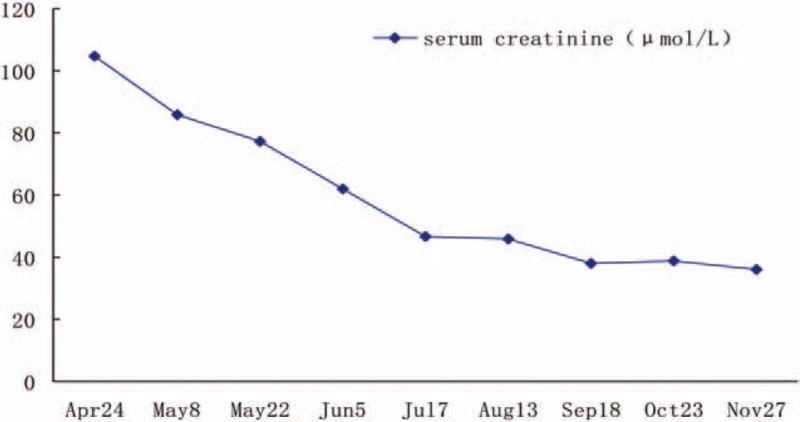
Interventions: The patient was treated with a 1mg vitamin B12 intramuscular injection daily for 4 days after which the dose was then adjusted to a 1mg intramuscular injection twice a week. At the same time, the girl was given levocarnitine, betaine, folic acid, along with supportive treatment.
Outcomes: After treated by vitamin B12 for 10 days, the patient condition significantly improved, Follow-up results showed complete recovery of hemoglobin and renal function.
Lessons: Although the majority of MMA onset from neurological damage, our case illustrates that partial CblC-type MMA can onset with severe metabolic aHUS. On the basis of chronic thrombotic microangiopathy (TMA)-induced renal damage, it can be complicated by acute hemolytic lesions. MMA should be considered in those patients with unclear microangiopathic hemolytic anemia accompany significant megaloblastic degeneration in bone marrow. We should pay attention to the causes and adopt a reasonable treatment strategy.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Late-onset renal TMA and tubular injury in cobalamin C disease: a report of three cases and literature review.BMC Nephrol. 2024 Oct 10;25(1):340. doi: 10.1186/s12882-024-03774-w. BMC Nephrol. 2024. PMID: 39390411 Free PMC article. Review.
-
The roles of homocysteinemia and methylmalonic acidemia in kidney injury in atypical hemolytic uremic syndrome caused by cobalamin C deficiency.Pediatr Nephrol. 2022 Jun;37(6):1415-1418. doi: 10.1007/s00467-021-05372-6. Epub 2021 Dec 2. Pediatr Nephrol. 2022. PMID: 34854955 Free PMC article.
-
Isolated subacute combined degeneration in late-onset cobalamin C deficiency in children: Two case reports and literature review.Medicine (Baltimore). 2019 Sep;98(39):e17334. doi: 10.1097/MD.0000000000017334. Medicine (Baltimore). 2019. PMID: 31574870 Free PMC article.
-
The MMACHC variant c.158T>C: Mild clinical and biochemical phenotypes and marked hydroxocobalamin response in cblC patients.Mol Genet Metab. 2024 May;142(1):108345. doi: 10.1016/j.ymgme.2024.108345. Epub 2024 Feb 10. Mol Genet Metab. 2024. PMID: 38387306
-
Combined methylmalonic acidemia and homocystinuria, cblC type. I. Clinical presentations, diagnosis and management.J Inherit Metab Dis. 2012 Jan;35(1):91-102. doi: 10.1007/s10545-011-9364-y. Epub 2011 Jul 12. J Inherit Metab Dis. 2012. PMID: 21748409 Free PMC article. Review.
Cited by
-
Late-onset renal TMA and tubular injury in cobalamin C disease: a report of three cases and literature review.BMC Nephrol. 2024 Oct 10;25(1):340. doi: 10.1186/s12882-024-03774-w. BMC Nephrol. 2024. PMID: 39390411 Free PMC article. Review.
-
Clinical, phenotypic and genetic landscape of case reports with genetically proven inherited disorders of vitamin B12 metabolism: A meta-analysis.Cell Rep Med. 2022 Jul 19;3(7):100670. doi: 10.1016/j.xcrm.2022.100670. Epub 2022 Jun 27. Cell Rep Med. 2022. PMID: 35764087 Free PMC article.
-
Pharmacological Management of Atypical Hemolytic Uremic Syndrome in Pediatric Patients: Current and Future.Paediatr Drugs. 2023 Mar;25(2):193-202. doi: 10.1007/s40272-022-00555-6. Epub 2023 Jan 13. Paediatr Drugs. 2023. PMID: 36637720 Free PMC article.
-
Rare cause of coronary artery ectasia in children: A case report of methylmalonic acidemia with hyperhomocysteinemia.Front Pediatr. 2022 Jul 22;10:917734. doi: 10.3389/fped.2022.917734. eCollection 2022. Front Pediatr. 2022. PMID: 35935352 Free PMC article.
-
Clinical Findings, Radiological Characteristics, and Treatment Options of Spontaneous and Secondary Intracranial Hypotension: A Single-Center Experience in Turkey.Cureus. 2024 Aug 21;16(8):e67439. doi: 10.7759/cureus.67439. eCollection 2024 Aug. Cureus. 2024. PMID: 39310496 Free PMC article.
References
-
- Morel CF, Lerner-Ellis JP, Rosenblatt DS. Combined methylmalonic aciduria and homocystinuria (cblC): phenotype-genotype correlations and ethnic-specific observations. Mol Genet Metab 2006;88:315–21. - PubMed
-
- Hörster F, Hoffmann GF. Pathophysiology, diagnosis, and treatment of methylmalonic aciduria-recent advances and new challenges. Pediatr Nephrol 2004;19:1071–4. - PubMed
-
- Talarico V, Aloe M, Monzani A, et al. Hemolytic uremic syndrome in children. Minerva Pediatr 2016;68:441–55. - PubMed
-
- Akashi Y, Yoshizawa N, Oshima S, et al. Hemolytic uremic syndrome without hemolytic anemia: a case report. Clin Nephrol 1994;42:90–4. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
