

Survival and complications of stereotactic radiosurgery: A systematic review of stereotactic radiosurgery for newly diagnosed and recurrent high-grade gliomas
- PMID: 29068998
- PMCID: PMC5671831
- DOI: 10.1097/MD.0000000000008293
Survival and complications of stereotactic radiosurgery: A systematic review of stereotactic radiosurgery for newly diagnosed and recurrent high-grade gliomas
Abstract
Background: Utilization of stereotactic radiosurgery (SRS) for treatment of high-grade gliomas (HGGs) has been slowly increasing with variable reported success rates.
Objective: Systematic review of the available data to evaluate the efficacy of SRS as a treatment for HGG with regards to median overall survival (OS) and progression-free survival (PFS), in addition to ascertaining the rate of radiation necrosis and other SRS-related major neurological complications.
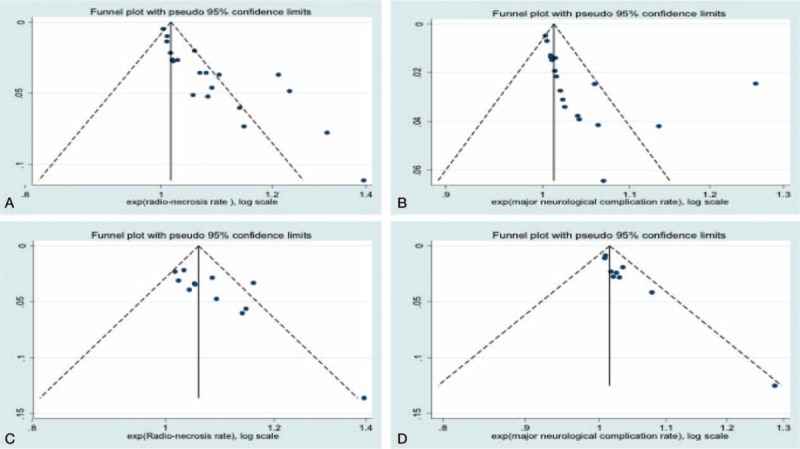
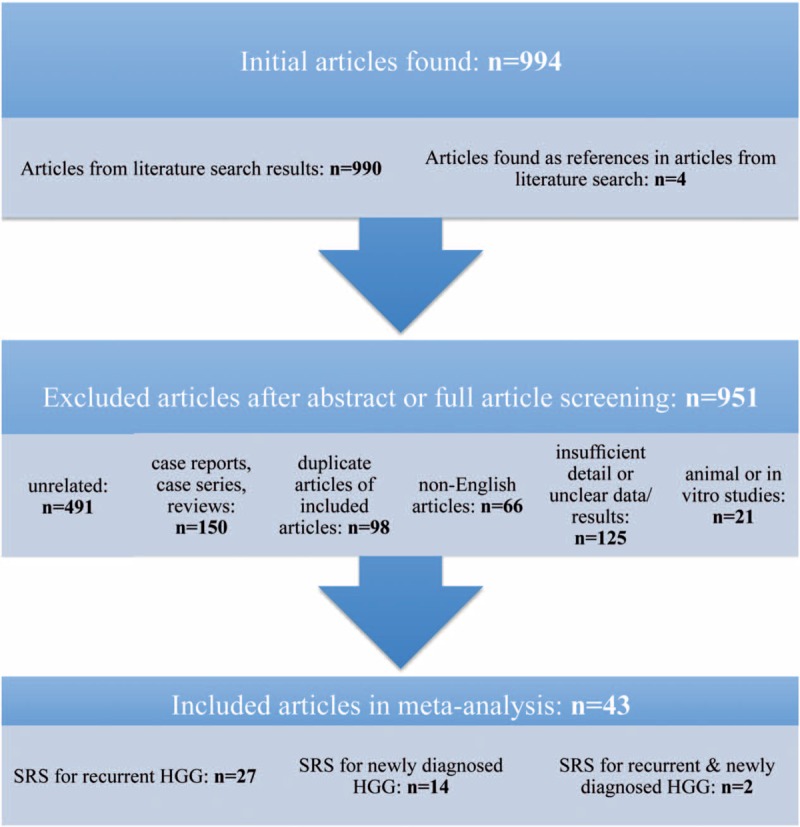
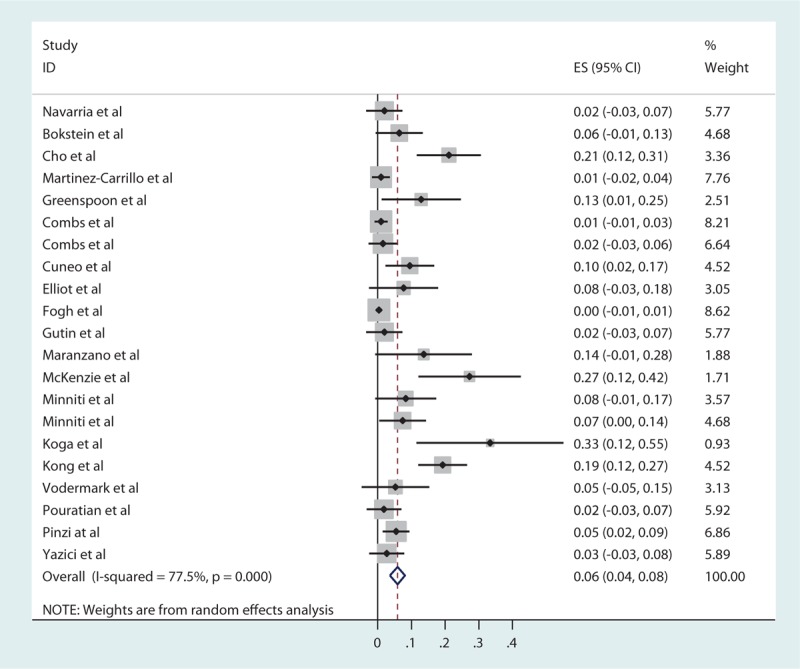
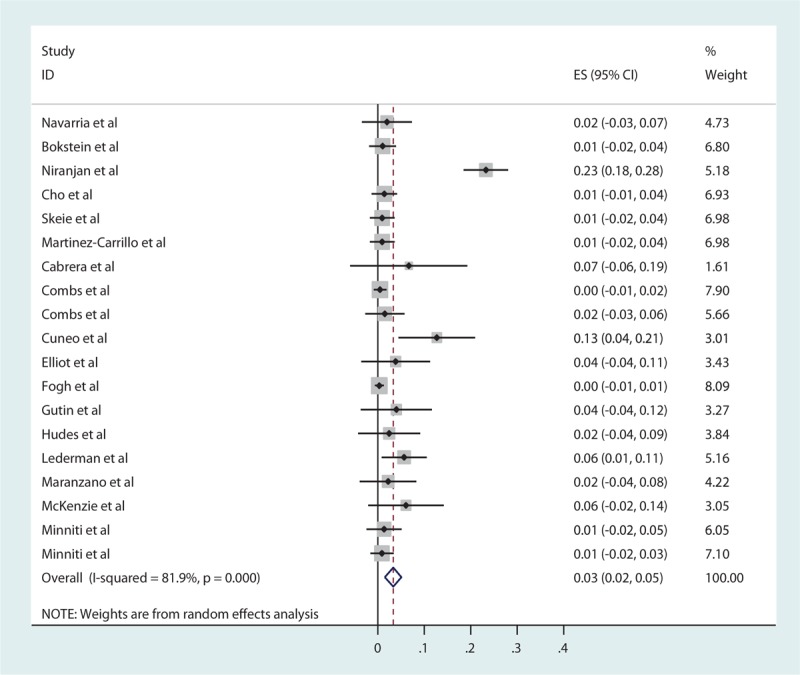
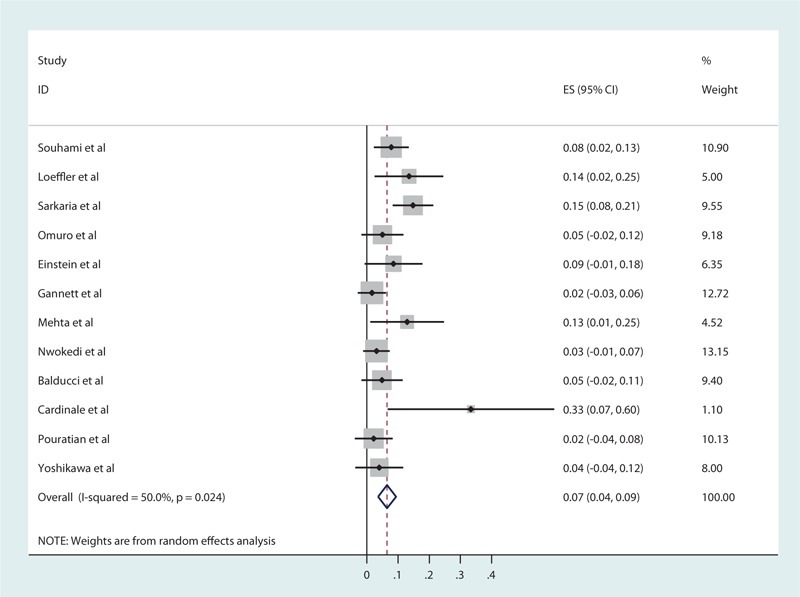
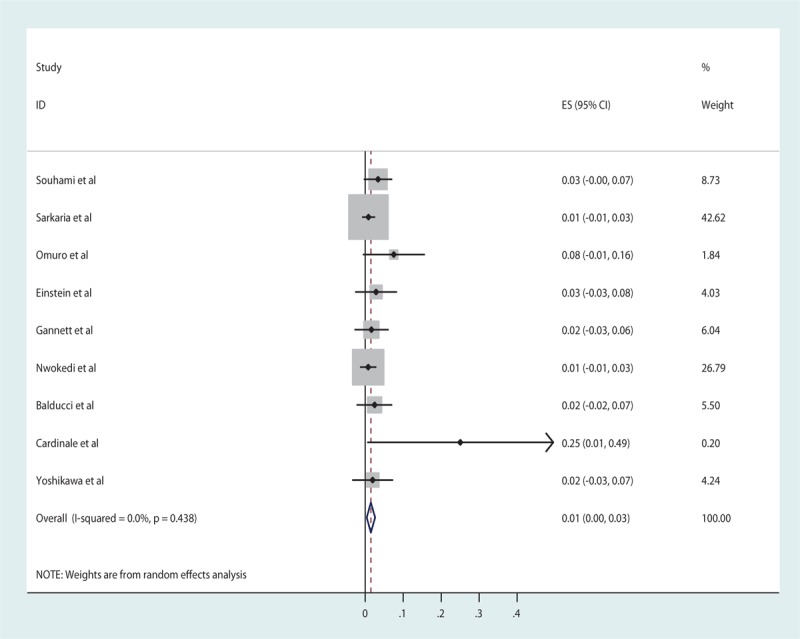
Methods: Literature searches were performed for publications from 1992 to 2016. The pooled estimates of median PFS and median OS were calculated as a weighted estimate of population medians. Meta-analyses of published rates of radiation necrosis and other major neurological complications were also performed.
Results: Twenty-nine studies reported the use of SRS for recurrent HGG, and 16 studies reported the use of SRS for newly diagnosed HGG. For recurrent HGG, the pooled estimates of median PFS and median OS were 5.42 months (3-16 months) and 20.19 months (9-65 months), respectively; the pooled radiation necrosis rate was 5.9% (0-44%); and the pooled estimates of major neurological complications rate was 3.3% (0-23%). For newly diagnosed HGG, the pooled estimates of median PFS and median OS were 7.89 months (5.5-11 months) and 16.87 months (9.5-33 months) respectively; the pooled radiation necrosis rate was 6.5% (0-33%); and the pooled estimates of other major neurological complications rate was 1.5% (0-25%).
Conclusion: Our results suggest that SRS holds promise as a relatively safe treatment option for HGG. In terms of efficacy at this time, there are inadequate data to support routine utilization of SRS as the standard of care for newly diagnosed or recurrent HGG. Further studies should be pursued to define more clearly the therapeutic role of SRS.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Prisco FE, Weltman E, de Hanriot RM, et al. Radiosurgical boost for primary high-grade gliomas. J Neurooncol 2002;57:151–60. - PubMed
-
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 2016;131:803–20. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
