

Diagnostic value of the corrected QT difference between leads V1 and V6 in patients with acute pulmonary thromboembolism
- PMID: 29069044
- PMCID: PMC5671877
- DOI: 10.1097/MD.0000000000008430
Diagnostic value of the corrected QT difference between leads V1 and V6 in patients with acute pulmonary thromboembolism
Abstract
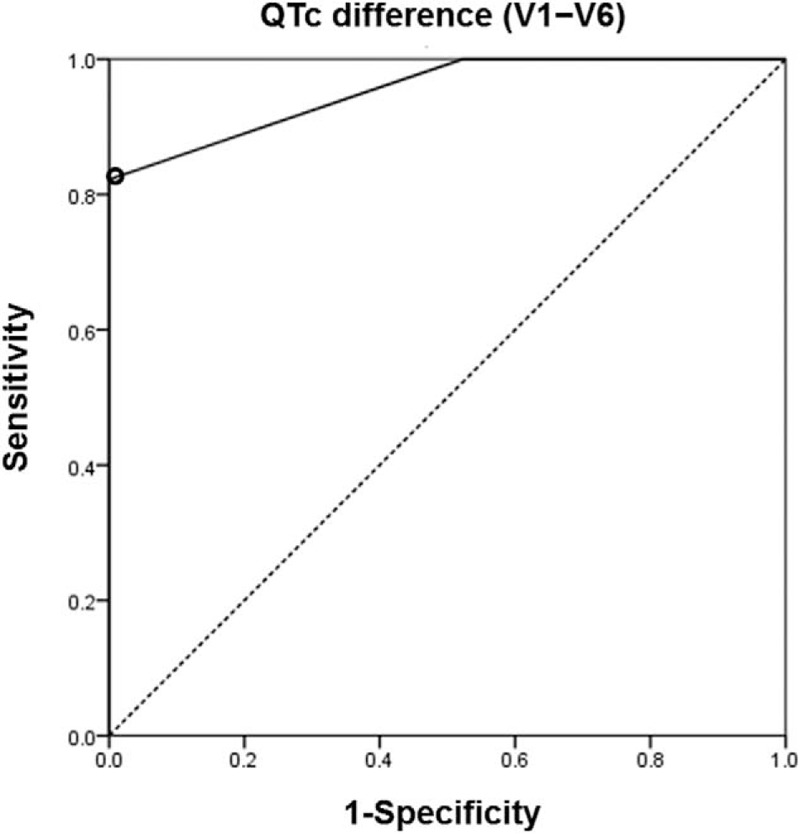
In acute pulmonary thromboembolism (PTE), right ventricular pressure overload impairs right-sided cardiac conduction and repolarization. We hypothesized that if heterogeneity of repolarization between right and left ventricles occurs in acute PTE, there would be the difference of repolarization between them. Therefore, we aimed to evaluate the diagnostic value of corrected QT interval (QTc) difference between leads V1 and V6 (V1 - V6) in patients with acute PTE.A total of 89 patients with suspected acute PTE who underwent computed tomographic angiography (CTA) were enrolled from January to December 2015. PTE was identified by CTA. We compared electrocardiographic (ECG) parameters, especially QTc difference (V1 - V6) between patients with PTE and those without PTE.Acute PTE was finally diagnosed in 45 patients. Clinical situations including the chief complaint were not different between PTE and non-PTE groups. S1Q3T3, a traditional ECG marker, had no diagnostic value for acute PTE. Patients with PTE had a significantly longer mean QTc in V1 (454.6 ± 44.3 vs 417.5 ± 31.3 ms, P < .001) and larger QTc difference (V1 - V6) (34.8 ± 30.5 vs -12.5 ± 16.6 ms, P < .001) than non-PTE controls. QTc difference (V1 - V6) was negative in all patients without PTE. PTE patients had a higher prevalence of T wave inversion in leads III (51.1% vs 29.5%, P = .038) and V1 (82.2% vs 38.6%, P < .001). A QTc difference (V1 - V6) of ≥20 ms identified PTE with 82.2% sensitivity, 100.0% specificity, and 100.0% positive predictive value.QTc difference (V1 - V6) had an excellent diagnostic value for differentiating patients with and without acute PTE.
Conflict of interest statement
The authors report no conflicts of interest.
Figures


References
-
- Carson JL, Kelley MA, Duff A, et al. The clinical course of pulmonary embolism. N Engl J Med 1992;326:1240–5. - PubMed
-
- Niwa A, Nakamura M, Harada N, et al. Observational investigation of thrombolysis with the tissue-type plasminogen activator monteplase for acute pulmonary embolism in Japan. Circ J 2012;76:2471–80. - PubMed
-
- Fedullo PF, Tapson VF. Clinical practice. The evaluation of suspected pulmonary embolism. N Engl J Med 2003;349:1247–56. - PubMed
-
- Stein PD, Terrin ML, Hales CA, et al. Clinical, laboratory, roentgenographic, and electrocardiographic findings in patients with acute pulmonary embolism and no pre-existing cardiac or pulmonary disease. Chest 1991;100:598–603. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
