

First results of the Brazilian Registry of Percutaneous Left Atrial Appendage Closure
- PMID: 29069203
- PMCID: PMC5729780
- DOI: 10.5935/abc.20170150
First results of the Brazilian Registry of Percutaneous Left Atrial Appendage Closure
Abstract
Background: Left atrial appendage closure (LAAC) is an effective alternative to oral anticoagulation (OA) for the prevention of stroke in patients with non-valvular atrial fibrillation (NVAF).
Objective: To present the immediate results and late outcomes of patients submitted to LAAC and included in the Brazilian Registry of Percutaneous Left Atrial Appendage Closure.
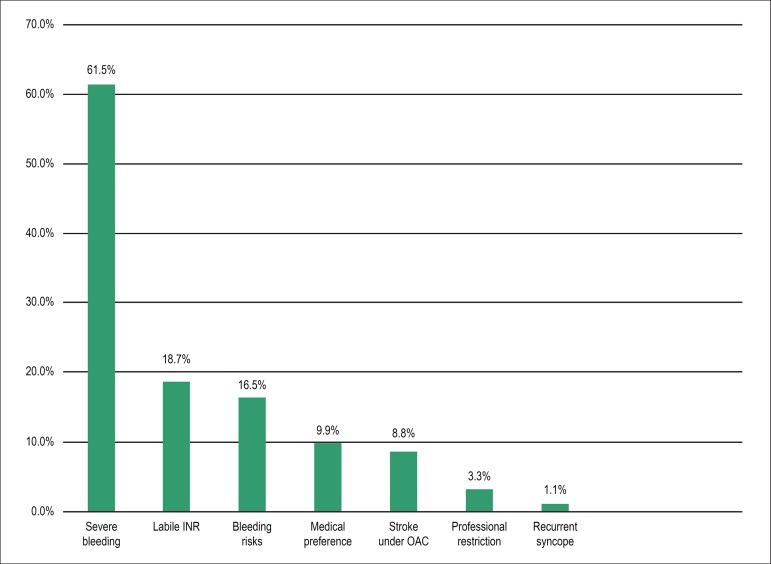
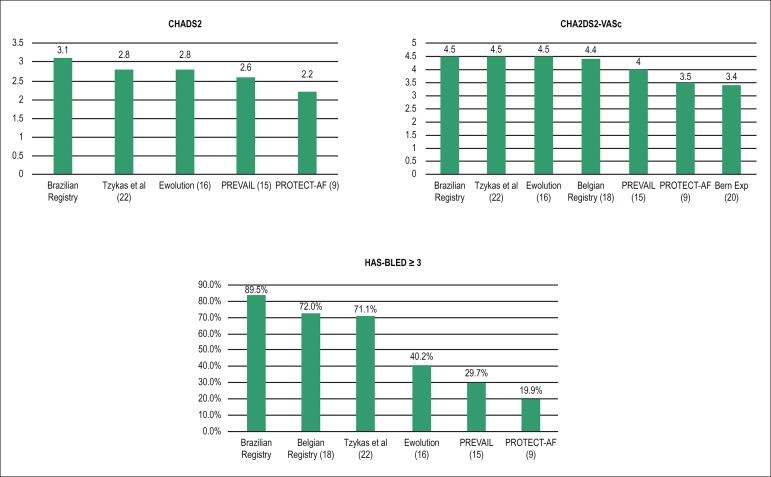
Methods: 91 patients with NVAF, high stroke risk (CHA2DS2VASc score = 4.5 ± 1.5) and restrictions to OAC (HAS-BLED score = 3.6 ± 1.0) underwent 92 LAAC procedures using either the Amplatzer cardiac plug or the Watchman device in 11 centers in Brazil, between late 2010 and mid 2016.
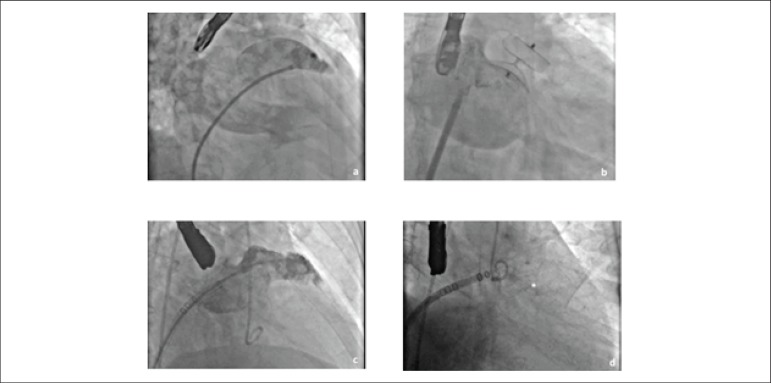
Results: Ninety-six devices were used (1.04 device/procedure, including an additional non-dedicated device), with a procedural success rate of 97.8%. Associated procedures were performed in 8.7% of the patients. Complete LAAC was obtained in 93.3% of the successful cases. In cases of incomplete closure, no residual leak was larger than 2.5 mm. One patient needed simultaneous implantation of 2 devices. There were 7 periprocedural major (5 pericardial effusions requiring pericardiocentesis, 1 non-dedicated device embolization and 1 coronary air embolism without sequelae) and 4 minor complications. After 128.6 patient-years of follow-up there were 3 deaths unrelated to the procedure, 2 major bleedings (one of them in a patient with an unsuccessful LAAC), thrombus formation over the device in 2 cases (both resolved after resuming OAC for 3 months) and 2 strokes (2.2%).
Conclusions: In this multicenter, real world registry, that included patients with NVAF and high thromboembolic and bleeding risks, LAAC effectively prevented stroke and bleeding when compared to the expected rates based on CHA2DS2VASc and HASBLED scores for this population. Complications rate of the procedure was acceptable considering the beginning of the learning curve of most of the involved operators.
Conflict of interest statement
Guérios EE is proctor for St. Jude Medical / Abbott for percutaneous left atrial appendage closure.
Figures

Comment in
-
Challenges For Percutaneous Left Atrial Appendage Closure: Imaging And Residual FlowReply.Arq Bras Cardiol. 2018 Jul;111(1):117. doi: 10.5935/abc.20180135. Arq Bras Cardiol. 2018. PMID: 30110056 Free PMC article. No abstract available.
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratns WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesotta, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114(2):119–125. doi: 10.1161/CIRCULATIONAHA.105.595140. Erratum in: Circulation. 2006;114(11):e498. - DOI - PubMed
-
- Stoddard MF, Dawkins PR, Prince CR, Ammash NM. Left atrial appendage thrombus is not uncommon in patients with acute atrial fibrillation and a recent embolic event: a transesophageal echocardiographic study. J Am Coll Cardiol. 1995;25(2):452–459. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
