

Monocyte and haematopoietic progenitor reprogramming as common mechanism underlying chronic inflammatory and cardiovascular diseases
- PMID: 29069365
- PMCID: PMC6174026
- DOI: 10.1093/eurheartj/ehx581
Monocyte and haematopoietic progenitor reprogramming as common mechanism underlying chronic inflammatory and cardiovascular diseases
Erratum in
-
Corrigendum to: Monocyte and haematopoietic progenitor reprogramming as common mechanism underlying chronic inflammatory and cardiovascular diseases.Eur Heart J. 2018 Jun 14;39(23):2182. doi: 10.1093/eurheartj/ehx703. Eur Heart J. 2018. PMID: 29190339 Free PMC article. No abstract available.
Abstract
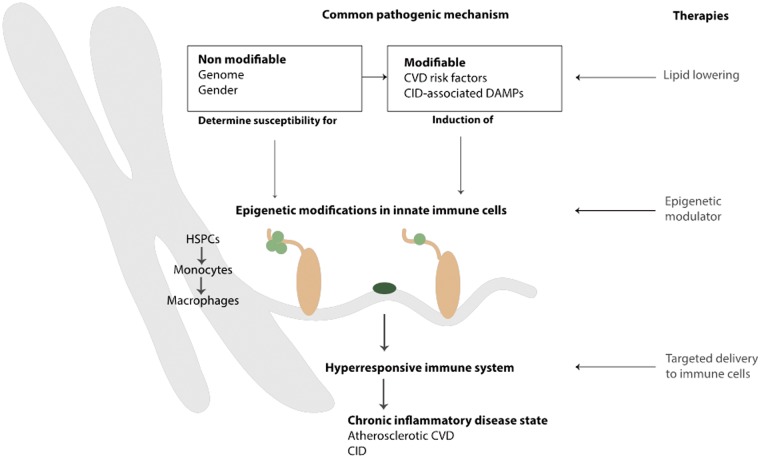
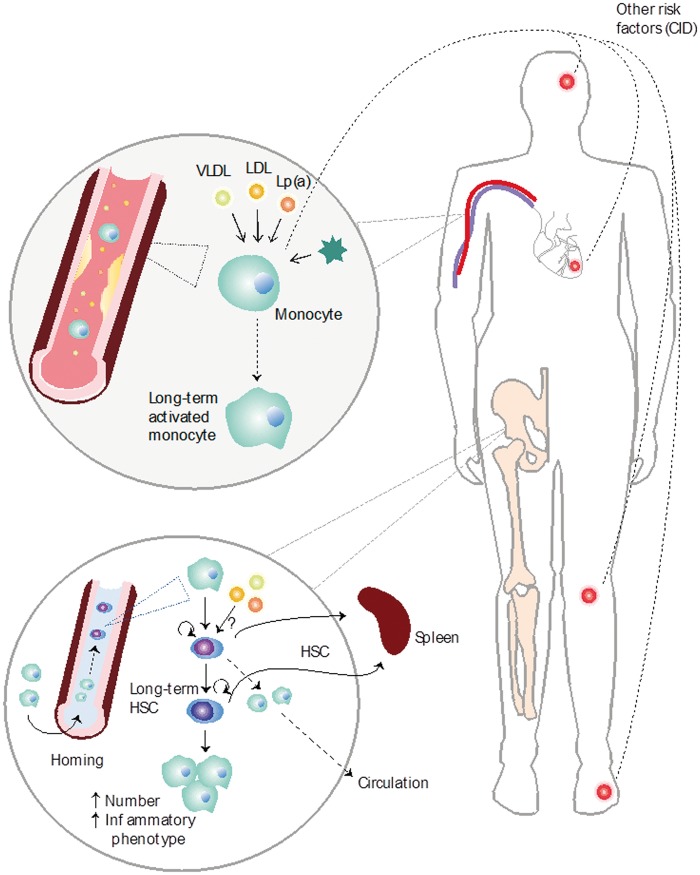
A large number of cardiovascular events are not prevented by current therapeutic regimens. In search for additional, innovative strategies, immune cells have been recognized as key players contributing to atherosclerotic plaque progression and destabilization. Particularly the role of innate immune cells is of major interest, following the recent paradigm shift that innate immunity, long considered to be incapable of learning, does exhibit immunological memory mediated via epigenetic reprogramming. Compelling evidence shows that atherosclerotic risk factors promote immune cell migration by pre-activation of circulating innate immune cells. Innate immune cell activation via metabolic and epigenetic reprogramming perpetuates a systemic low-grade inflammatory state in cardiovascular disease (CVD) that is also common in other chronic inflammatory disorders. This opens a new therapeutic area in which metabolic or epigenetic modulation of innate immune cells may result in decreased systemic chronic inflammation, alleviating CVD, and its co-morbidities.
Figures
References
-
- Alwan A, Armstrong T, Bettcher D.. Global status report on noncummunicable diseases. Geneva, Switzerland: World Health Organization; 2011.
-
- Libby P. Inflammation in atherosclerosis. Nature 2002;420:868–874. - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, Finkelstein EA, Hong Y, Johnston SC, Khera A, Lloyd-Jones DM, Nelson SA, Nichol G, Orenstein D, Wilson PWF, Woo YJ; American Heart Association Advocacy Coordinating Committee, Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Clinical Cardiology, Council on Epidemiology and Prevention, Council on Arteriosclerosis, Thrombosis and Vascular Biology, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Cardiovascular Nursing, Council on the Kidney in Cardiovascular Disease, Council on Cardiovascular Surgery and Anesthesia, and Interdisciplinary Council on Quality of Care and Outcomes Research . Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 2011;123:933–944. - PubMed
-
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005;352:1685–1695. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
