

High-resolution three-dimensional late gadolinium-enhanced cardiac magnetic resonance imaging to identify the underlying substrate of ventricular arrhythmia
- PMID: 29069369
- PMCID: PMC6140447
- DOI: 10.1093/europace/eux278
High-resolution three-dimensional late gadolinium-enhanced cardiac magnetic resonance imaging to identify the underlying substrate of ventricular arrhythmia
Abstract
Aims: Cardiac magnetic resonance (CMR) is recommended as a second-line method to diagnose ventricular arrhythmia (VA) substrate. We assessed the diagnostic yield of CMR including high-resolution late gadolinium-enhanced (LGE) imaging.
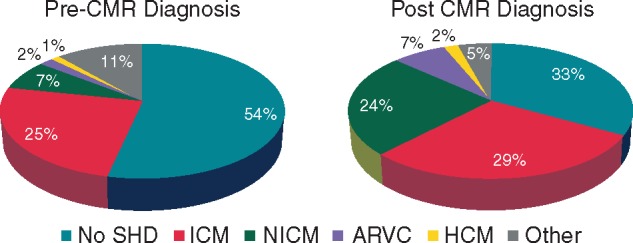
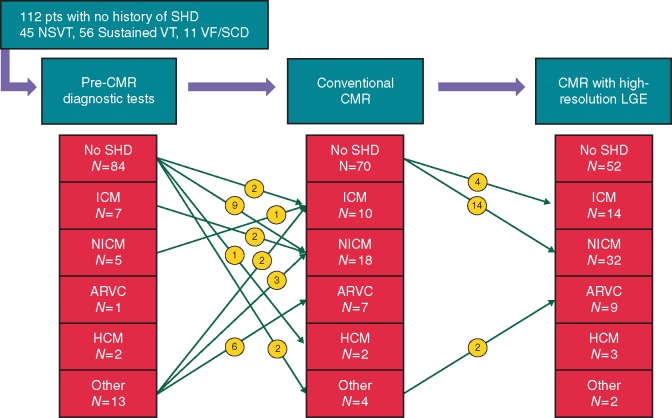
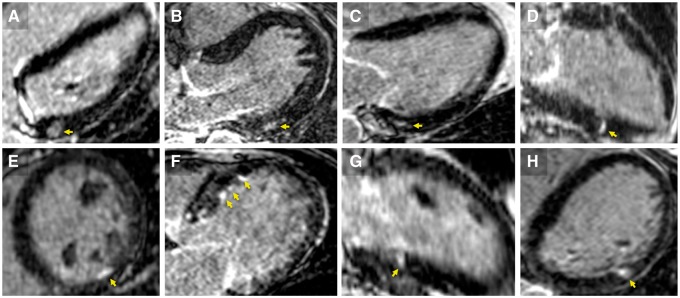
Methods and results: Consecutive patients with sustained ventricular tachycardia (VT), non-sustained VT (NSVT), or ventricular fibrillation/aborted sudden death (VF/SCD) underwent a non-CMR diagnostic workup according to current guidelines, and CMR including LGE imaging with both a conventional breath-held and a free-breathing method enabling higher spatial resolution (HR-LGE). The diagnostic yield of CMR was compared with the non-CMR workup, including the incremental value of HR-LGE. A total of 157 patients were enrolled [age 54 ± 17 years; 75% males; 88 (56%) sustained VT, 52 (33%) NSVT, 17 (11%) VF/SCD]. Of these, 112 (71%) patients had no history of structural heart disease (SHD). All patients underwent electrocardiography and echocardiography, 72% coronary angiography, and 51% exercise testing. Pre-CMR diagnoses were 84 (54%) no SHD, 39 (25%) ischaemic cardiomyopathy (ICM), 11 (7%) non-ischaemic cardiomyopathy (NICM), 3 (2%) arrhythmogenic right ventricular cardiomyopathy (ARVC), 2 (1%) hypertrophic cardiomyopathy (HCM), and 18 (11%) other. CMR modified these diagnoses in 48 patients (31% of all and 43% of those with no SHD history). New diagnoses were 9 ICM, 28 NICM, 8 ARVC, 1 HCM, and 2 other. CMR modified therapy in 19 (12%) patients. In patients with no SHD after non-CMR tests, SHD was found in 32 of 84 (38%) patients. Eighteen of these patients showed positive HR-LGE and negative conventional LGE. Thus, HR-LGE significantly increased the CMR detection of SHD (17-38%, P < 0.001).
Conclusion: CMR including HR-LGE imaging has high diagnostic value in patients with VAs. This has major prognostic and therapeutic implications, particularly in patients with negative pre-CMR workup.
Figures
Similar articles
-
Does stress perfusion imaging improve the diagnostic accuracy of late gadolinium enhanced cardiac magnetic resonance for establishing the etiology of heart failure?BMC Cardiovasc Disord. 2017 Apr 8;17(1):98. doi: 10.1186/s12872-017-0529-y. BMC Cardiovasc Disord. 2017. PMID: 28390413 Free PMC article.
-
Image Integration to Guide Catheter Ablation in Scar-Related Ventricular Tachycardia.J Cardiovasc Electrophysiol. 2016 Jun;27(6):699-708. doi: 10.1111/jce.12963. Epub 2016 Apr 5. J Cardiovasc Electrophysiol. 2016. PMID: 26918883
-
Absence of late gadolinium enhancement on cardiac magnetic resonance imaging in ventricular fibrillation and nonischemic cardiomyopathy.Pacing Clin Electrophysiol. 2018 Sep;41(9):1109-1115. doi: 10.1111/pace.13426. Epub 2018 Jul 16. Pacing Clin Electrophysiol. 2018. PMID: 29931686
-
Prediction of ventricular arrhythmias using cardiovascular magnetic resonance.Eur Heart J Cardiovasc Imaging. 2013 Jun;14(6):518-25. doi: 10.1093/ehjci/jes302. Epub 2013 Jan 16. Eur Heart J Cardiovasc Imaging. 2013. PMID: 23324829 Review.
-
Prognostic Value of LGE-CMR in HCM: A Meta-Analysis.JACC Cardiovasc Imaging. 2016 Dec;9(12):1392-1402. doi: 10.1016/j.jcmg.2016.02.031. Epub 2016 Jul 20. JACC Cardiovasc Imaging. 2016. PMID: 27450876 Review.
Cited by
-
Whole-Heart High-Resolution Late Gadolinium Enhancement: Techniques and Clinical Applications.J Magn Reson Imaging. 2022 Apr;55(4):967-987. doi: 10.1002/jmri.27732. Epub 2021 Jun 21. J Magn Reson Imaging. 2022. PMID: 34155715 Free PMC article. Review.
-
Management of Ventricular Arrhythmias in Heart Failure.Curr Heart Fail Rep. 2023 Aug;20(4):237-253. doi: 10.1007/s11897-023-00608-y. Epub 2023 May 25. Curr Heart Fail Rep. 2023. PMID: 37227669 Review.
-
Twenty-five years of catheter ablation of ventricular tachycardia: a look back and a look forward.Europace. 2023 Aug 2;25(9):euad225. doi: 10.1093/europace/euad225. Europace. 2023. PMID: 37622589 Free PMC article.
-
Role of 3-Dimensional Architecture of Scar and Surviving Tissue in Ventricular Tachycardia: Insights From High-Resolution Ex Vivo Porcine Models.Circ Arrhythm Electrophysiol. 2018 Jun;11(6):e006131. doi: 10.1161/CIRCEP.117.006131. Circ Arrhythm Electrophysiol. 2018. PMID: 29880529 Free PMC article.
-
Usefulness of three-dimensional echocardiography for the assessment of ventricular function in children: Comparison with cardiac magnetic resonance, with a focus on patients with arrhythmia.Cardiol J. 2021;28(4):549-557. doi: 10.5603/CJ.a2019.0026. Epub 2019 Mar 26. Cardiol J. 2021. PMID: 30912575 Free PMC article.
References
-
- Zipes DP, Wellens HJ.. Sudden cardiac death. Circulation 1998;98:2334–51. - PubMed
-
- Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, et al.ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Europace 2006;8:746–837. - PubMed
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al.2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Europace 2015;17:1601–87. - PubMed
-
- White JA, Fine NM, Gula L, Yee R, Skanes A, Klein G. et al. Utility of cardiovascular magnetic resonance in identifying substrate for malignant ventricular arrhythmias. Circ Cardiovasc Imaging 2012;5:12–20. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
