

Do attributes of persons with chronic kidney disease differ in low-income and middle-income countries compared with high-income countries? Evidence from population-based data in six countries
- PMID: 29071132
- PMCID: PMC5640036
- DOI: 10.1136/bmjgh-2017-000453
Do attributes of persons with chronic kidney disease differ in low-income and middle-income countries compared with high-income countries? Evidence from population-based data in six countries
Abstract
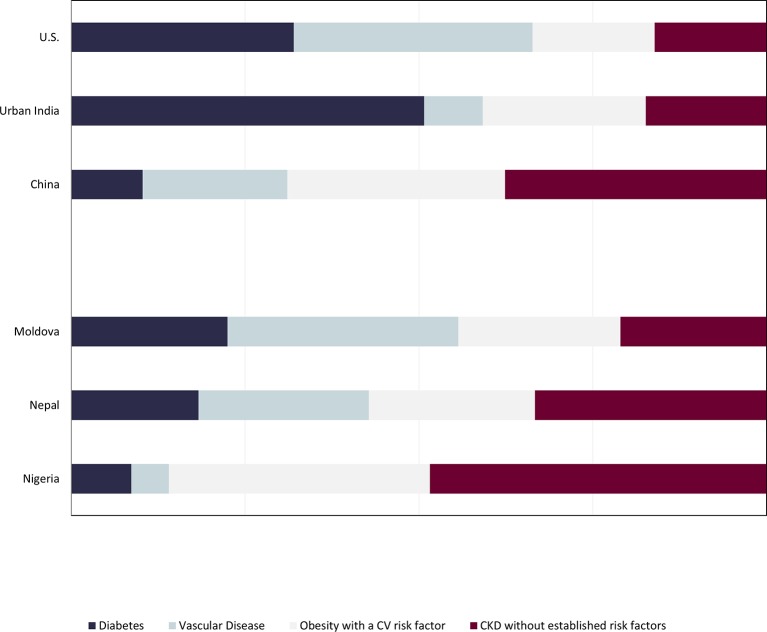
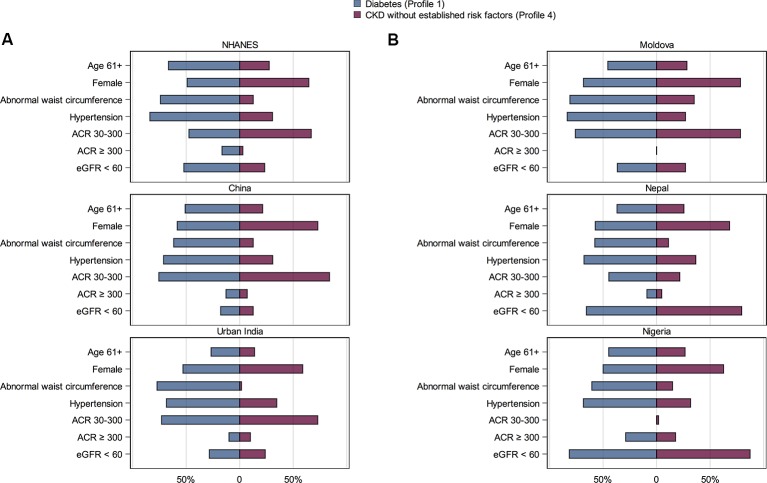
Kidney biopsies to elucidate the cause of chronic kidney disease (CKD) are performed in a minority of persons with CKD living in high-income countries, since associated conditions-that is, diabetes mellitus, vascular disease or obesity with pre-diabetes, prehypertension or dyslipidaemia-can inform management targeted at slowing CKD progression in a majority. However, attributes of CKD may differ substantially among persons living in low-income and middle-income countries (LMICs). We used data from population or community-based studies from five LMICs (China, urban India, Moldova, Nepal and Nigeria) to determine what proportion of persons with CKD living in diverse regions fit one of the three major clinical profiles, with data from the US National Health Nutrition and Examination Survey as reference. In the USA, urban India and Moldova, 79.0%-83.9%; in China and Nepal, 62.4%-66.7% and in Nigeria, 51.6% persons with CKD fit one of three established risk profiles. Diabetes was most common in urban India and vascular disease in Moldova (50.7% and 33.2% of persons with CKD in urban India and Moldova, respectively). In Nigeria, 17.8% of persons with CKD without established risk factors had albuminuria ≥300 mg/g, the highest proportion in any country. While the majority of persons with CKD in LMICs fit into one of three established risk profiles, the proportion of persons who have CKD without established risk factors is higher than in the USA. These findings can inform tailored CKD detection and management systems and highlight the importance of studying potential causes and outcomes of CKD without established risk factors in LMICs.
Keywords: cross-sectional survey; epidemiology; indices of health and disease and standardisation of rates.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Anand STB, Remuzzi G, Riella M, et al. Kidney disease : Dorairaj P, Gaziano T, Anand S, disease control priorities (volume 5 c, respiratory, and related disorders). 3rd India: the world bank, 2016. http://dcp-3.org/cvd
-
- United States renal data system. 2013. USRDS 2013 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States: CKD in the general population. National institutes of health. Bethesda, MD: national institutes of health, national institute of diabetes and digestive and kidney diseases.
-
- Australian institute of health and welfare. An overview of chronic kidney disease in Australia. Canberra: Australian institute of health and welfare, 2009.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources