

Evaluation of Military Use of Tranexamic Acid and Associated Thromboembolic Events
- PMID: 29071337
- PMCID: PMC5838717
- DOI: 10.1001/jamasurg.2017.3821
Evaluation of Military Use of Tranexamic Acid and Associated Thromboembolic Events
Abstract
Importance: Since publication of the CRASH-2 and MATTERs studies, the US military has included tranexamic acid (TXA) in clinical practice guidelines. While TXA was shown to decrease mortality in trauma patients requiring massive transfusion, improper administration and increased risk of venous thromboembolism remain a concern.
Objective: To determine the appropriateness of TXA administration by US military medical personnel based on current Joint Trauma System clinical practice guidelines and to determine if TXA administration is associated with venous thromboembolism.
Design, setting, and participants: This cohort study of US military casualties in US military combat support hospitals in Afghanistan and a single US-based tertiary military treatment facility within the continental United States was conducted from 2011 to 2015, with follow-up through initial hospitalization and readmissions.
Exposures: Data collected for all patients included demographic information as well as Injury Severity Score; receipt of blood products, TXA, and/or a massive transfusion; and admission hemodynamics.
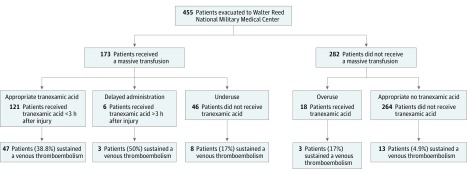
Main outcomes and measures: Variance from guidelines in TXA administration and venous thromboembolism. Tranexamic acid overuse was defined as a hemodynamically stable patient receiving TXA but not a massive transfusion, underuse was defined as a patient receiving a massive transfusion but not TXA, and TXA administration was considered delayed when given more than 3 hours after injury.
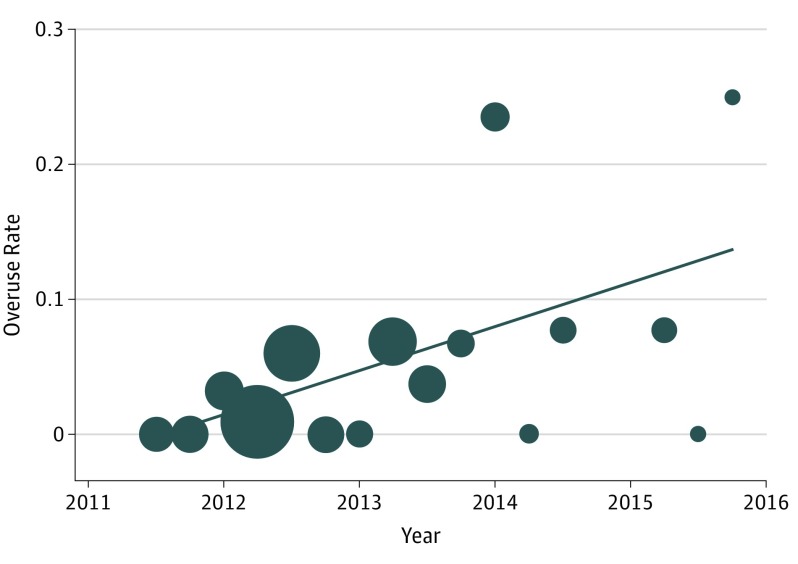
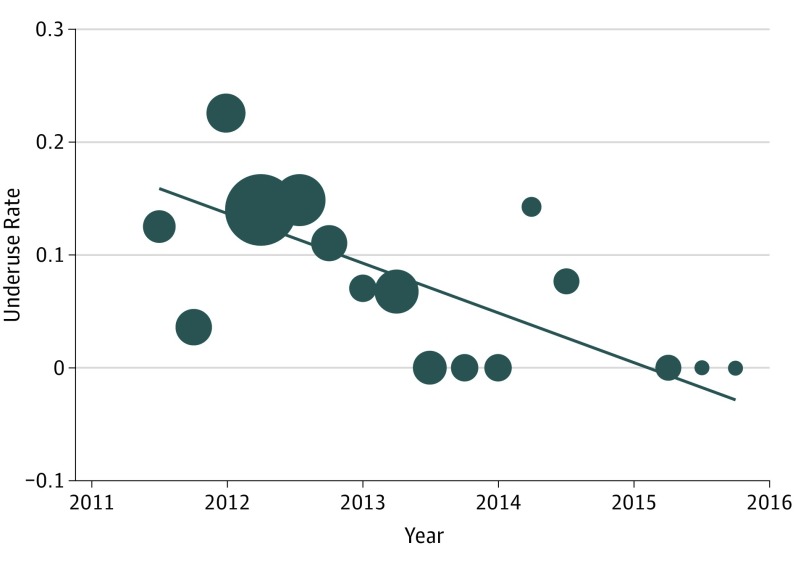
Results: Of the 455 identified patients, 443 (97.4%) were male, and the mean (SD) age was 25.3 (4.8) years. A total of 173 patients (38.0%) received a massive transfusion, and 139 (30.5%) received TXA in theater. Overuse occurred in 18 of 282 patients (6.4%) and underuse in 46 of 173 (26.6%) receiving massive transfusions, and delayed administration was found in 6 of 145 patients (4.3%) receiving TXA. Overuse increased at 3.3% per quarter (95% CI, 4.0-9.9; P < .001; R2 = 0.340) and underuse decreased at -4.4% per quarter (95% CI, -4.5 to -3.6; P < .001; R2 = 0.410). Tranexamic acid administration was an independent risk factor for venous thromboembolism (odds ratio, 2.58; 95% CI, 1.20-5.56; P = .02).
Conclusions and relevance: Military medical personnel decreased missed opportunities to appropriately use TXA but also increased overuse. In addition, TXA administration was an independent risk factor for venous thromboembolism. A reevaluation of the use of TXA in combat casualties should be undertaken.
Conflict of interest statement
Figures
Comment in
-
Does Tranexamic Acid Cause Venous Thromboembolism After Trauma?: Who Cares, If It Saves Lives?JAMA Surg. 2018 Feb 1;153(2):175-176. doi: 10.1001/jamasurg.2017.3855. JAMA Surg. 2018. PMID: 29071350 No abstract available.
References
-
- Shakur H, Roberts I, Bautista R, et al. ; CRASH-2 trial collaborators . Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23-32. - PubMed
-
- Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) study. Arch Surg. 2012;147(2):113-119. - PubMed
-
- US Army Institute of Surgical Research Damage control resuscitation (CPG ID: 18). http://www.usaisr.amedd.army.mil/cpgs/DamageControlResuscitation_03Feb20... Accessed January 10, 2017.
-
- National Association of Emergency Medical Technicians. Tactical combat casualty care guidelines for medical personnel guidelines and curriculum. http://www.naemt.org/education/TCCC/guidelines_curriculum. Accessed January 10, 2017.
-
- Roberts I, Shakur H, Afolabi A, et al. ; CRASH-2 collaborators . The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-1101, 1101.e1-1101.e2. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
