

Prognostic Effect and Longitudinal Hemodynamic Assessment of Borderline Pulmonary Hypertension
- PMID: 29071338
- PMCID: PMC5814998
- DOI: 10.1001/jamacardio.2017.3882
Prognostic Effect and Longitudinal Hemodynamic Assessment of Borderline Pulmonary Hypertension
Abstract
Importance: Pulmonary hypertension (PH) is diagnosed by a mean pulmonary arterial pressure (mPAP) value of at least 25 mm Hg during right heart catheterization (RHC). While several studies have demonstrated increased mortality in patients with mPAP less than that threshold, little is known about the natural history of borderline PH.
Objective: To test the hypothesis that patients with borderline PH have decreased survival compared with patients with lower mPAP and frequently develop overt PH and to identify clinical correlates of borderline PH.
Design, setting, and participants: Retrospective cohort study from 1998 to 2014 at Vanderbilt University Medical Center, comprising all patients undergoing routine RHC for clinical indication. We extracted demographics, clinical data, invasive hemodynamics, echocardiography, and vital status for all patients. Patients with mPAP values of 18 mm Hg or less, 19 to 24 mm Hg, and at least 25 mm Hg were classified as reference, borderline PH, and PH, respectively.
Exposures: Mean pulmonary arterial pressure.
Main outcome and measures: Our primary outcome was all-cause mortality after adjusting for clinically relevant covariates in a Cox proportional hazards model. Our secondary outcome was the diagnosis of overt PH in patients initially diagnosed with borderline PH. Both outcomes were determined prior to data analysis.
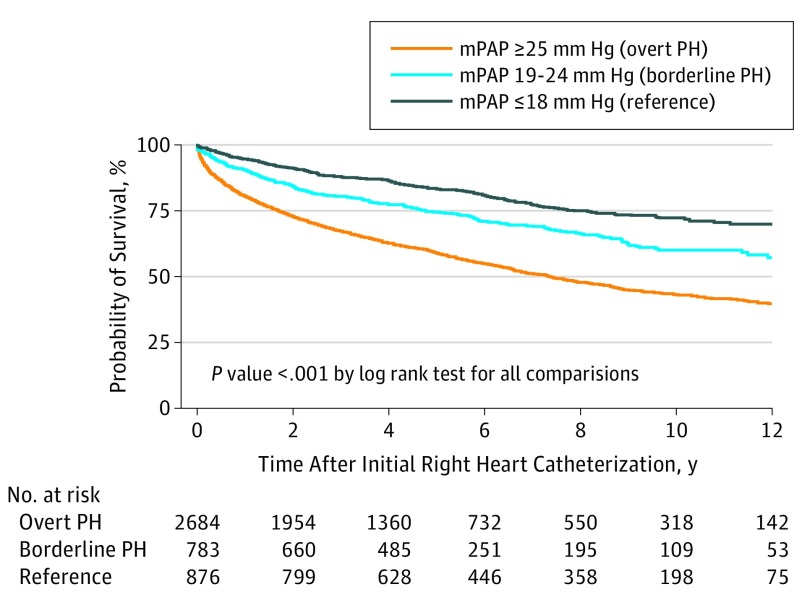
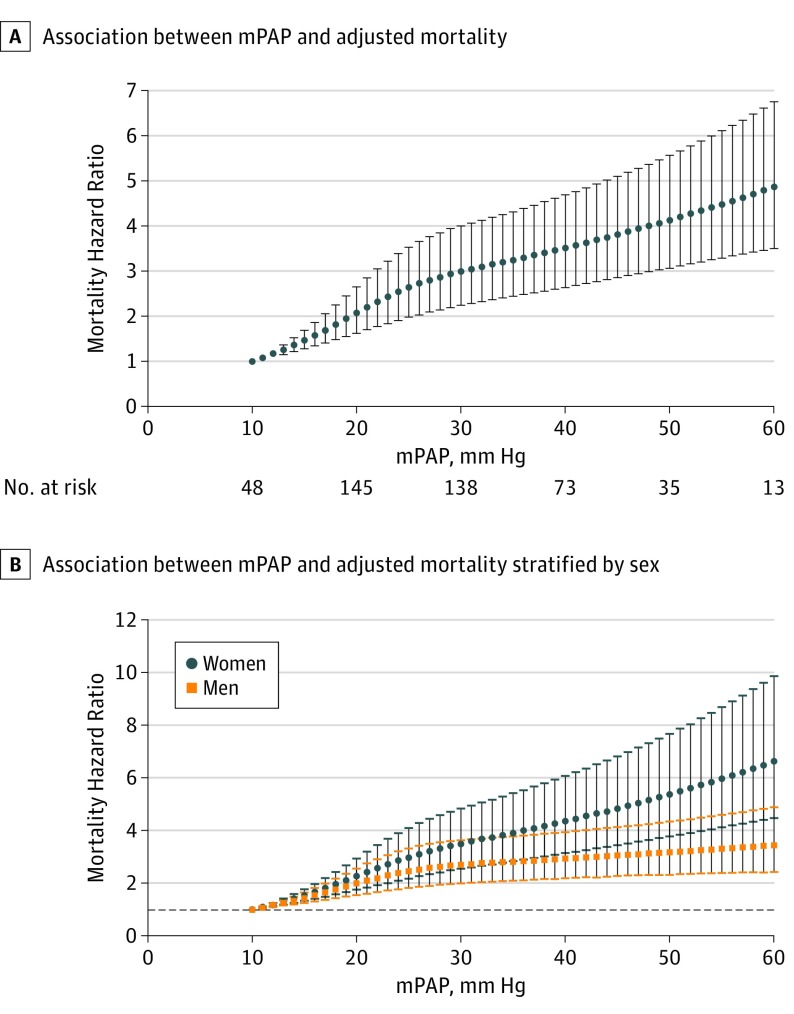
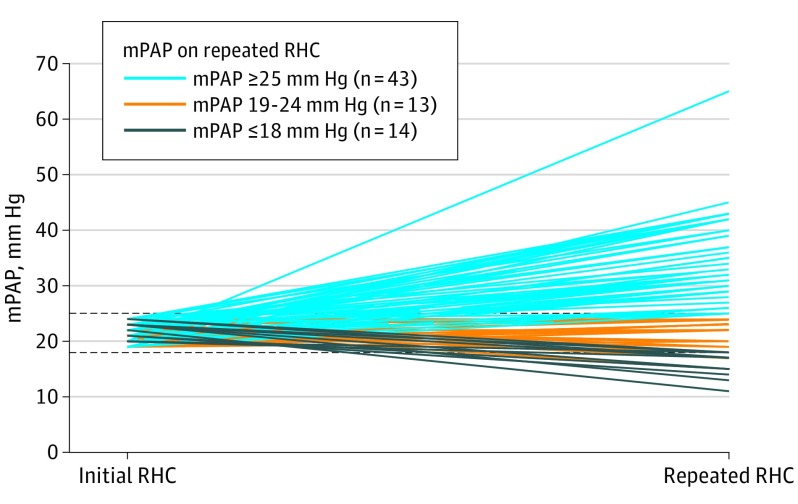
Results: We identified 4343 patients (mean [SD] age, 59 [15] years, 51% women, and 86% white) among whom the prevalence of PH and borderline PH was 62% and 18%, respectively. Advanced age, features of the metabolic syndrome, and chronic heart and lung disease were independently associated with a higher likelihood of borderline PH compared with reference patients in a logistic regression model. After adjusting for 34 covariates in a Cox proportional hazards model, borderline PH was associated with increased mortality compared with reference patients (hazard ratio, 1.31; 95% CI, 1.04-1.65; P = .001). The hazard of death increased incrementally with higher mPAP, without an observed threshold. In the 70 patients with borderline PH who underwent a repeated RHC, 43 (61%) had developed overt PH, with a median increase in mPAP of 5 mm Hg (interquartile range, -1 to 11 mm Hg; P < .001).
Conclusions and relevance: Borderline PH is common in patients undergoing RHC and is associated with significant comorbidities, progression to overt PH, and decreased survival. Small increases in mPAP, even at values currently considered normal, are independently associated with increased mortality. Prospective studies are warranted to determine whether early intervention or closer monitoring improves clinical outcomes in these patients.
Conflict of interest statement
Figures
References
-
- Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25)(suppl):D34-D41. - PubMed
-
- Seeger W, Adir Y, Barberà JA, et al. Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol. 2013;62(25)(suppl):D109-D116. - PubMed
-
- Vachiéry JL, Adir Y, Barberà JA, et al. Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol. 2013;62(25)(suppl):D100-D108. - PubMed
-
- Hatano SST. Primary Pulmonary Hypertension: Report on a WHO Meeting. Geneva, Switzerland; World Health Organization; 1975.
-
- Kovacs G, Berghold A, Scheidl S, Olschewski H. Pulmonary arterial pressure during rest and exercise in healthy subjects: a systematic review. Eur Respir J. 2009;34(4):888-894. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
