

Fragments of e-Cadherin as Biomarkers of Non-erosive Reflux Disease
- PMID: 29071486
- PMCID: PMC5823739
- DOI: 10.1007/s10620-017-4815-4
Fragments of e-Cadherin as Biomarkers of Non-erosive Reflux Disease
Abstract
Background: Approximately, 20% of patients with heartburn and normal endoscopic findings do not symptomatically improve on proton pump inhibitor (PPI) therapy making diagnosis and treatment uncertain. A biomarker distinguishing PPI-responsive from PPI-refractory heartburn is desirable.
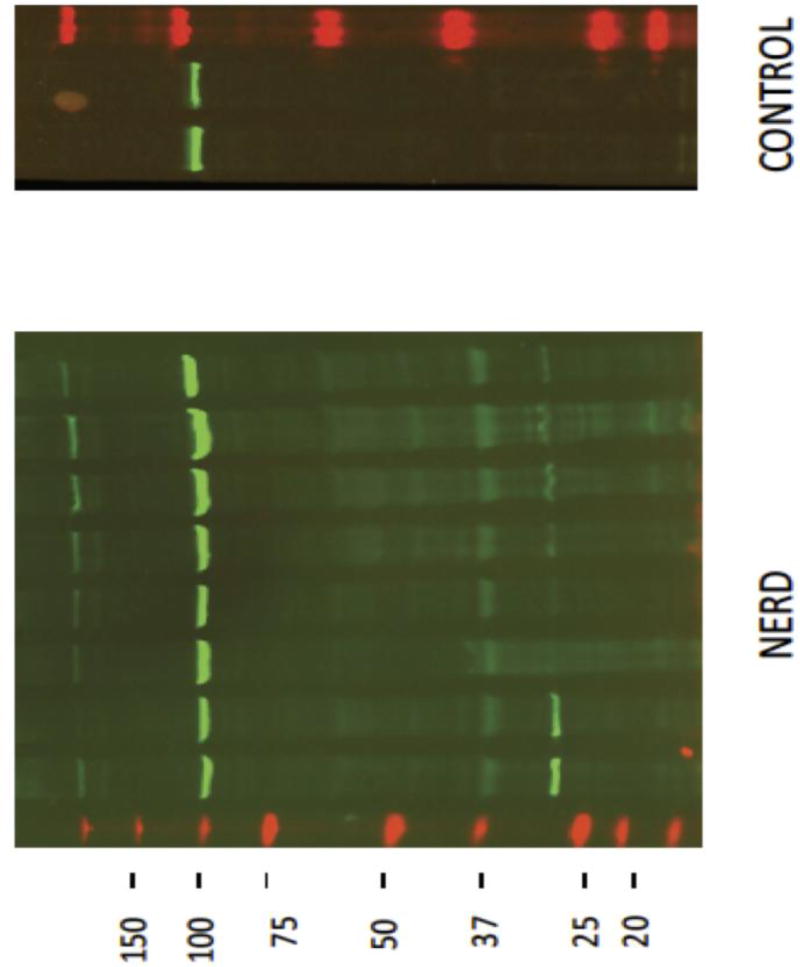
Aims: We performed a pilot study assessing whether carboxy(C)-terminal fragments (CTFs) of e-cadherin in esophageal biopsies or amino(N)-terminal fragments (NTFs) of e-cadherin in serum could serve this purpose.
Methods: Twenty-nine patients with endoscopy-negative heartburn had esophageal biopsies for CTFs on Western blot and blood for serum NTFs on ELISA. All patients received dexlansoprazole 30 mg daily for 4 weeks, and heartburn was assessed by daily diary entry. Post-treatment blood samples were obtained for serum NTFs. A control group without GERD symptoms (n = 6) had biopsies for CTFs and a second control group (n = 20) blood serum for serum NTFs.
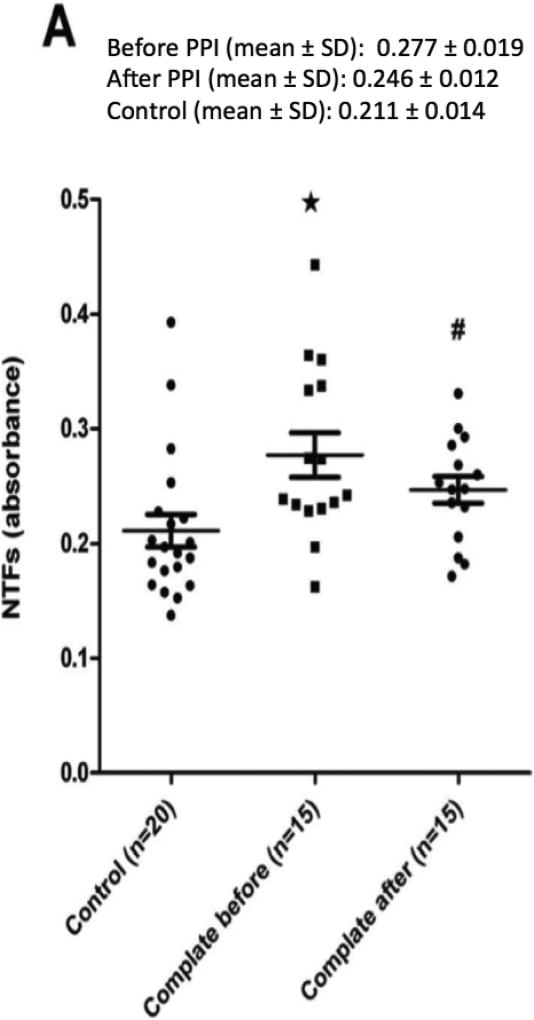
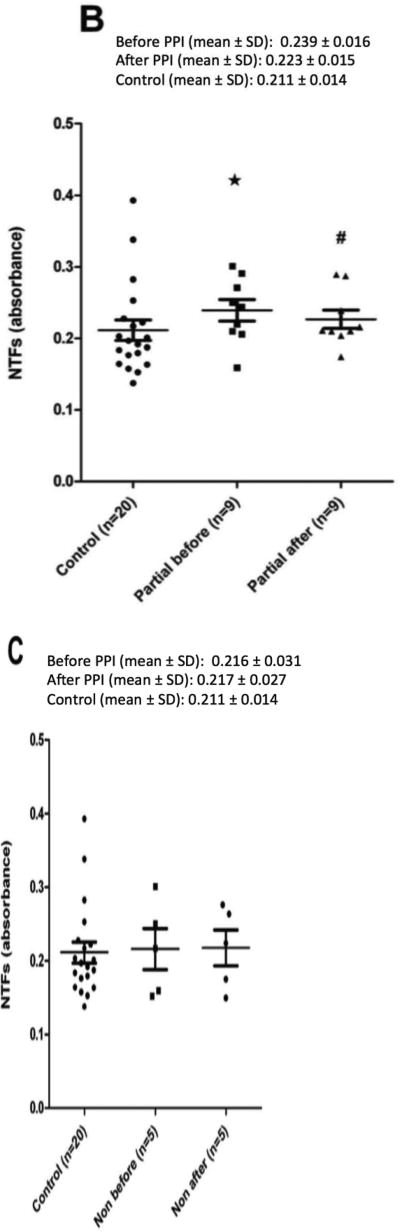
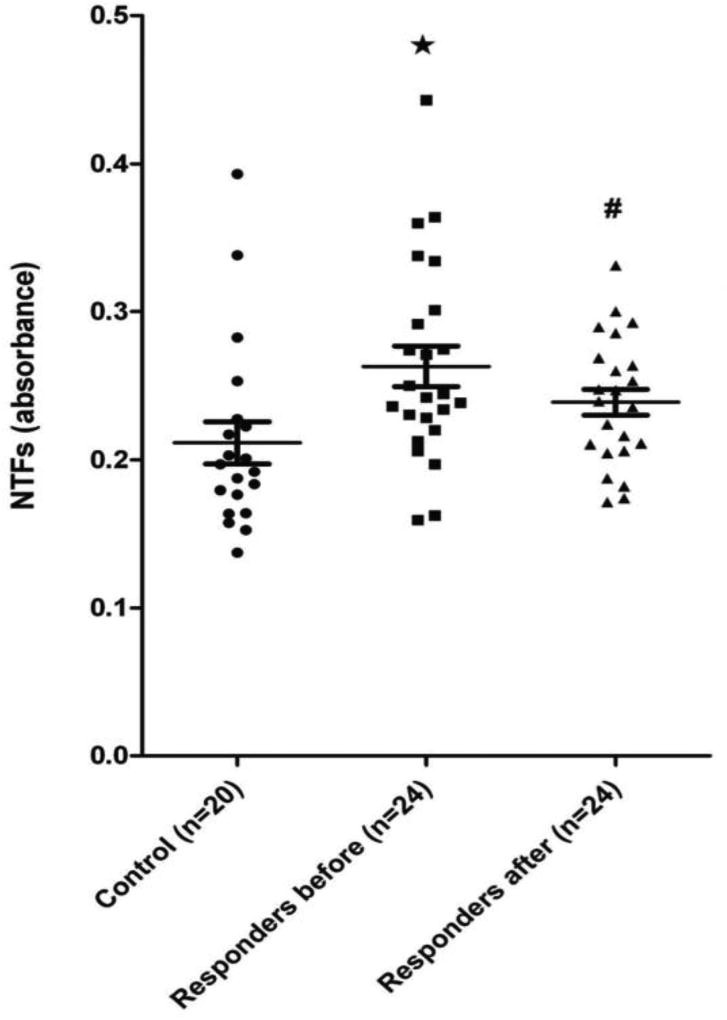
Results: Twenty-seven of 29 patients (93.1%) with endoscopy-negative heartburn, but 0 of 6 controls, were positive for CTFs. All patients and controls had measureable serum NTFs, but mean NTFs were significantly higher in those with PPI-responsive heartburn compared to those with PPI-refractory heartburn and controls. Following treatment, 24 of 29 (82.8) patients had relief of heartburn, which associated with a decline in mean NTFs compared to controls. NTFs in PPI-refractory patients (n = 5) were similar to controls before and after PPI therapy.
Conclusions: When heartburn responds to PPI, elevated serum NTFs decline to normal. These data suggest that cleaved products of e-cadherin may serve as biomarkers of NERD. Further data are needed to assess and confirm this concept.
Keywords: Dysphagia; Functional heartburn; Gastroesophageal reflux disease; Heartburn; Odynophagia.
Figures

Comment in
-
Revenge of the NERDs: Cadherin Fragments Differentiate Functional Heartburn from Non-erosive Reflux Disease.Dig Dis Sci. 2018 Mar;63(3):547-548. doi: 10.1007/s10620-017-4872-8. Dig Dis Sci. 2018. PMID: 29330729 No abstract available.
Similar articles
-
Cleavage of E-Cadherin Contributes to Defective Barrier Function in Neosquamous Epithelium.Dig Dis Sci. 2016 Nov;61(11):3169-3175. doi: 10.1007/s10620-016-4315-y. Epub 2016 Sep 22. Dig Dis Sci. 2016. PMID: 27659669 Free PMC article.
-
Algorithmic approach to patients presenting with heartburn and epigastric pain refractory to empiric proton pump inhibitor therapy.Dig Dis Sci. 2011 Oct;56(10):2871-8. doi: 10.1007/s10620-011-1708-9. Epub 2011 Apr 22. Dig Dis Sci. 2011. PMID: 21512760
-
Distinguishing the impact of dexlansoprazole on heartburn vs. regurgitation in patients with gastro-oesophageal reflux disease.Aliment Pharmacol Ther. 2013 Nov;38(10):1303-11. doi: 10.1111/apt.12504. Epub 2013 Sep 30. Aliment Pharmacol Ther. 2013. PMID: 24118079 Clinical Trial.
-
Untangling Nonerosive Reflux Disease From Functional Heartburn.Clin Gastroenterol Hepatol. 2021 Jul;19(7):1314-1326. doi: 10.1016/j.cgh.2020.03.057. Epub 2020 Apr 1. Clin Gastroenterol Hepatol. 2021. PMID: 32246998 Review.
-
Impedance-pH Monitoring for Diagnosis of Reflux Disease: New Perspectives.Dig Dis Sci. 2017 Aug;62(8):1881-1889. doi: 10.1007/s10620-017-4625-8. Epub 2017 May 26. Dig Dis Sci. 2017. PMID: 28550489 Review.
Cited by
-
Revenge of the NERDs: Cadherin Fragments Differentiate Functional Heartburn from Non-erosive Reflux Disease.Dig Dis Sci. 2018 Mar;63(3):547-548. doi: 10.1007/s10620-017-4872-8. Dig Dis Sci. 2018. PMID: 29330729 No abstract available.
-
Identification of Unique Transcriptomic Signatures and Hub Genes Through RNA Sequencing and Integrated WGCNA and PPI Network Analysis in Nonerosive Reflux Disease.J Inflamm Res. 2021 Nov 23;14:6143-6156. doi: 10.2147/JIR.S340452. eCollection 2021. J Inflamm Res. 2021. PMID: 34848992 Free PMC article.
References
-
- Locke GR, Talley NJ, Fett SL, et al. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112(5):1448–56. - PubMed
-
- El-Serag HB, Petersen NJ, Carter J, et al. Gastroesophageal reflux among different racial groups in the United States. Gastroenterology. 2004;126(7):1692–9. - PubMed
-
- Kahrilas PJ, Shaheen NJ, Vaezi MF. American Gastroenterological Association Medical Position Statement on the Management of Gastroesophageal Reflux Disease. Gastroenterology. 2008;135(4) - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
