

Merkel cell carcinoma
- PMID: 29072302
- PMCID: PMC6054450
- DOI: 10.1038/nrdp.2017.77
Merkel cell carcinoma
Abstract
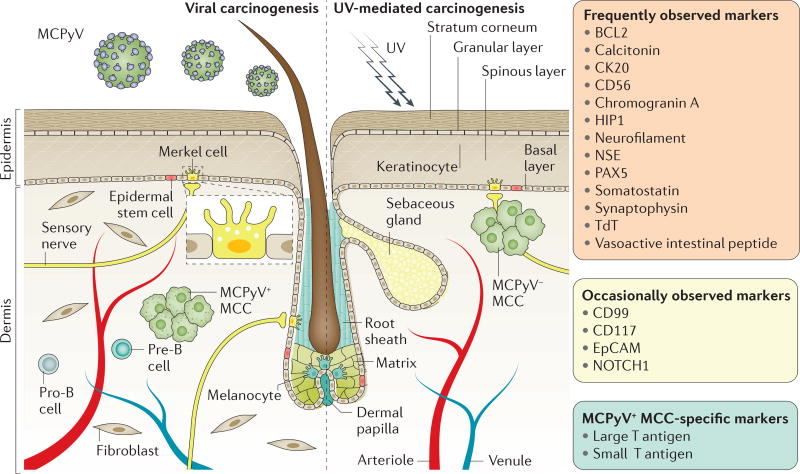
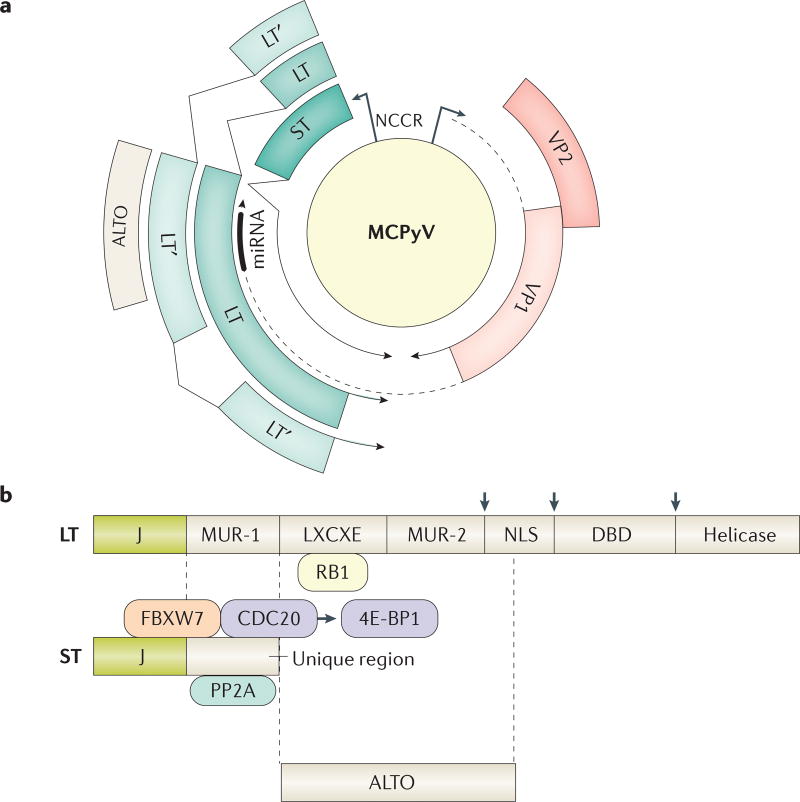
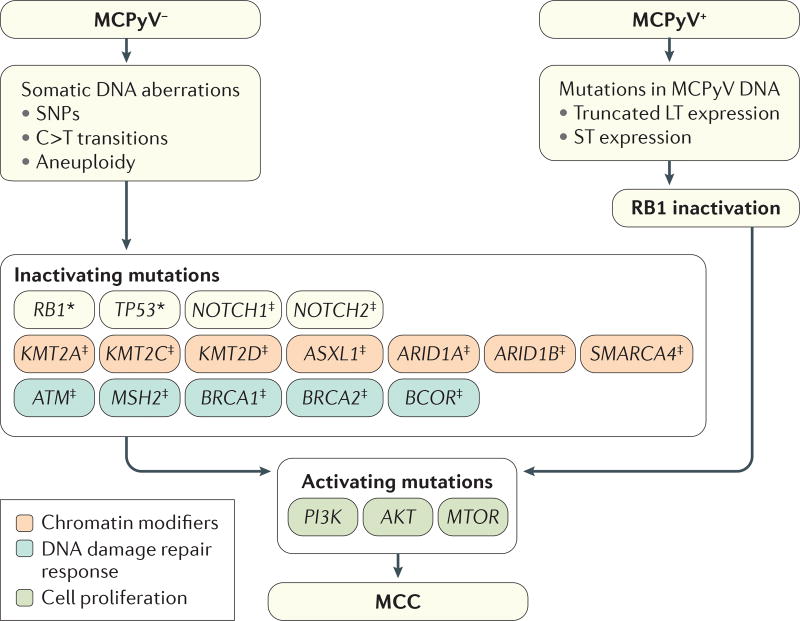
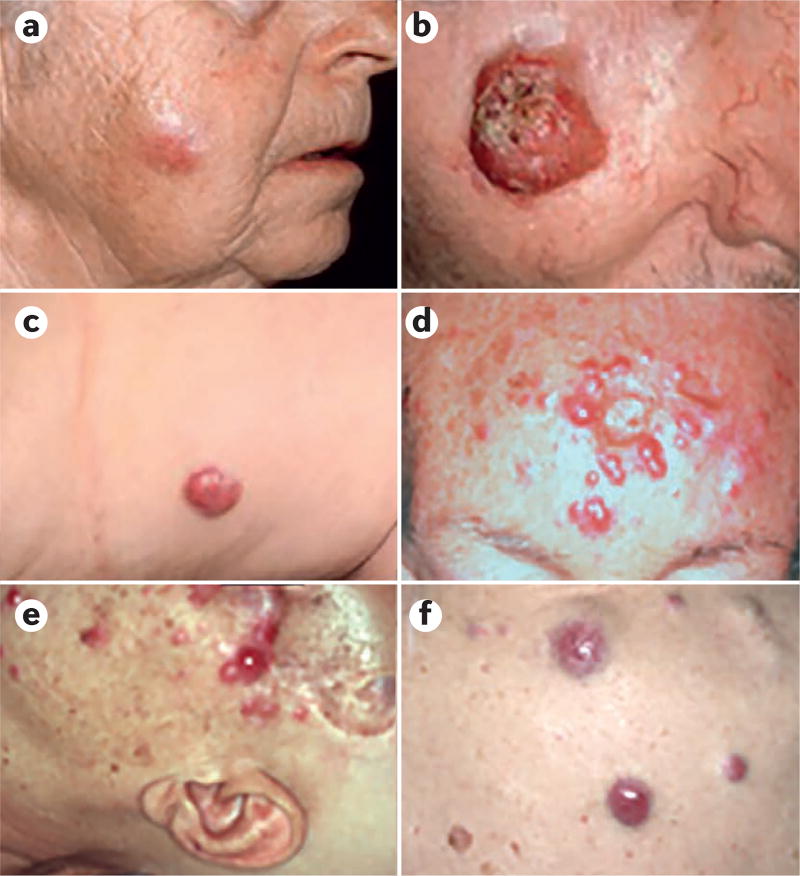
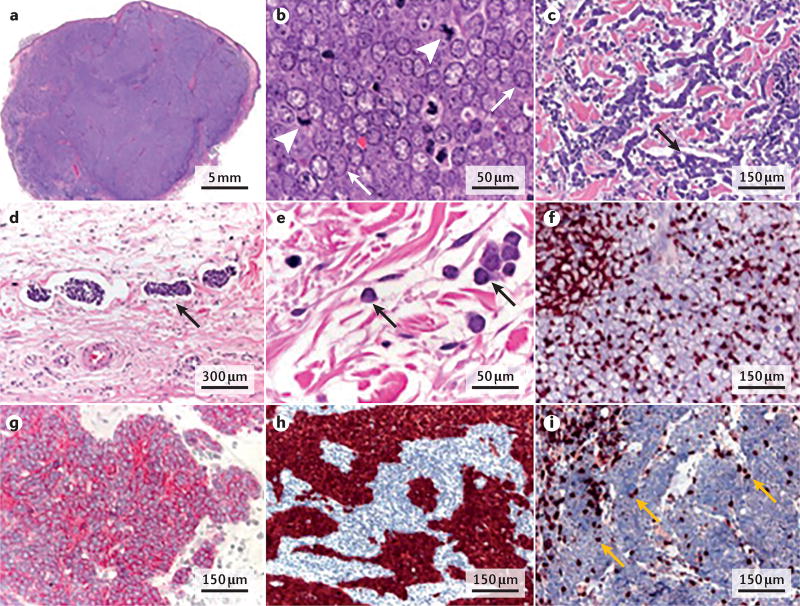
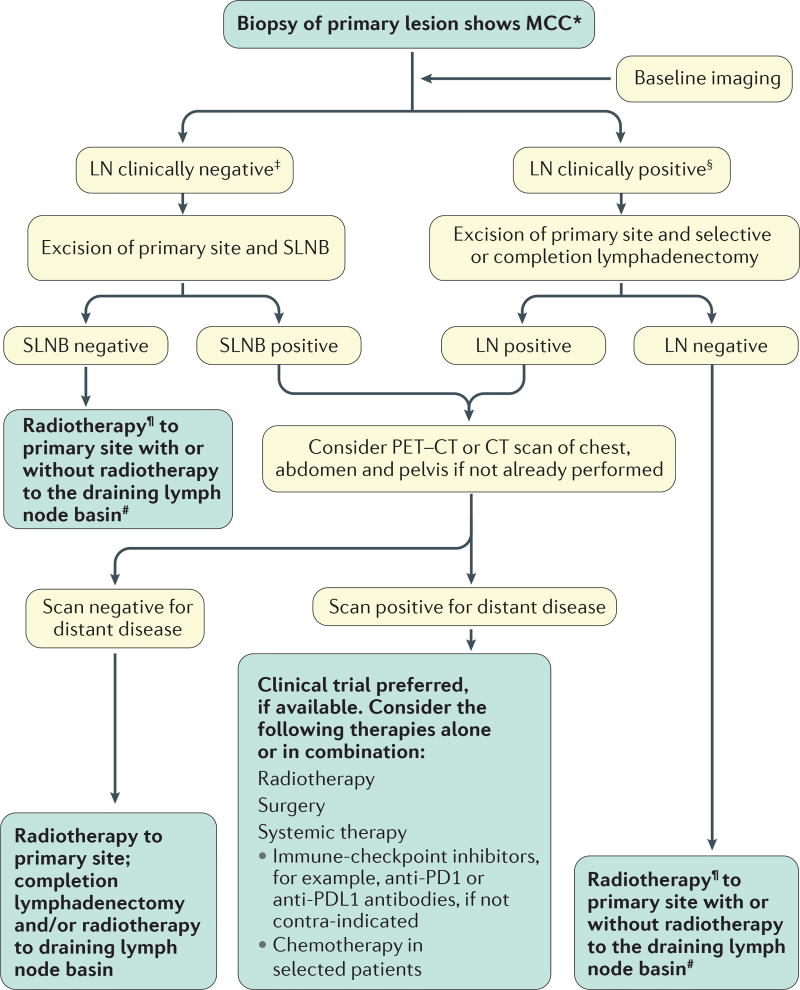
Merkel cell carcinoma (MCC) is a rare but highly aggressive skin cancer with neuroendocrine features. MCC pathogenesis is associated with either the presence of Merkel cell polyomavirus or chronic exposure to ultraviolet light (UV), which can cause a characteristic pattern of multiple DNA mutations. Notably, in the Northern hemisphere, the majority of MCC cases are of viral aetiology; by contrast, in areas with high UV exposure, UV-mediated carcinogenesis is predominant. The two aetiologies share similar clinical, histopathological and prognostic characteristics. MCC presents with a solitary cutaneous or subcutaneous nodule, most frequently in sun-exposed areas. In fact, UV exposure is probably involved in both viral-mediated and non-viral-mediated carcinogenesis, by contributing to immunosuppression or DNA damage, respectively. Confirmation of diagnosis relies on analyses of histological features and immunological marker expression profiles of the lesion. At primary diagnosis, loco-regional metastases are already present in ∼30% of patients. Excision of the tumour is the first-line therapy; if not feasible, radiotherapy can often effectively control the disease. Chemotherapy was the only alternative in advanced-stage or refractory MCC until several clinical trials demonstrated the efficacy of immune-checkpoint inhibitors.
Conflict of interest statement
A.S., L.C. and M.V. declare no competing interests.
Figures
References
-
- Toker C. Trabecular carcinoma of the skin. Arch. Dermatol. 1972;105:107–110. - PubMed
-
- Schrama D, et al. Merkel cell polyomavirus status is not associated with clinical course of Merkel cell carcinoma. J. Invest. Dermatol. 2011;131:1631–1638. - PubMed
-
- Becker JC, Schrama D, zur Hausen A. In: Rook’s Textbook of Dermatology. 9. Ch. 145. Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Vol. 12. John Wiley & Sons, Inc.; 2016.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
