

Flat epithelial atypia: conservative management of patients without residual microcalcifications post-vacuum-assisted breast biopsy
- PMID: 29072858
- PMCID: PMC5966211
- DOI: 10.1259/bjr.20170484
Flat epithelial atypia: conservative management of patients without residual microcalcifications post-vacuum-assisted breast biopsy
Abstract
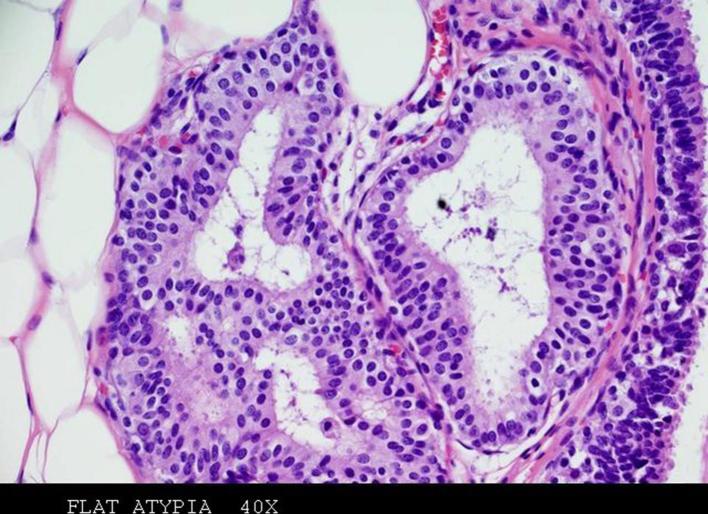
Objective: To determine the malignancy rate (defined in this study as stability or absence of malignancy developed on close imaging follow-up post-biopsy) of conservative management in patients with a vacuum-assisted breast biopsy (VAB) diagnosis of flat epithelial atypia (FEA), performed on single group of microcalcifications, completely removed during procedure.
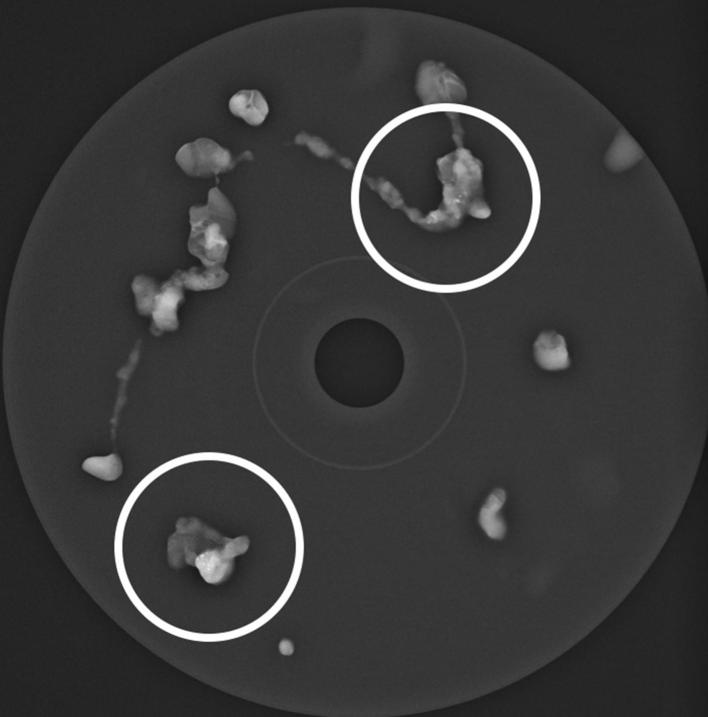
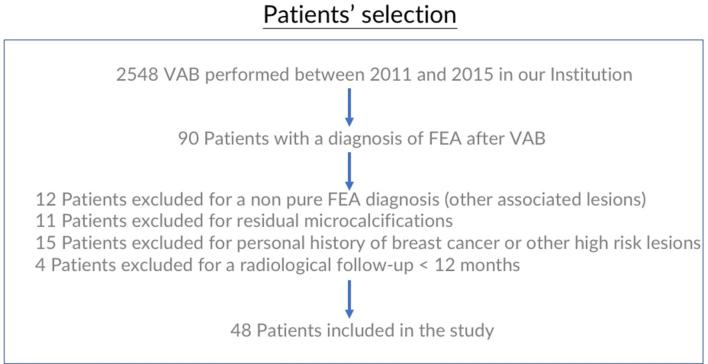
Methods: This is a retrospective, monocentric, observational study, approved by IRB. Inclusion criteria were: VAB performed on a single group of microcalcifications; the absence of residual calcifications post-VAB; diagnosis of isolated FEA as the most advanced proliferative lesion; radiological follow-up at least of 12 months. The personal history of breast cancer or other high-risk lesions was an exclusion criteria. The patients enrolled were conservatively managed, without surgical excision, through close follow-up: the first two mammographies performed with an interval of 6 months after biopsy, followed by annual mammographic and clinical checks.
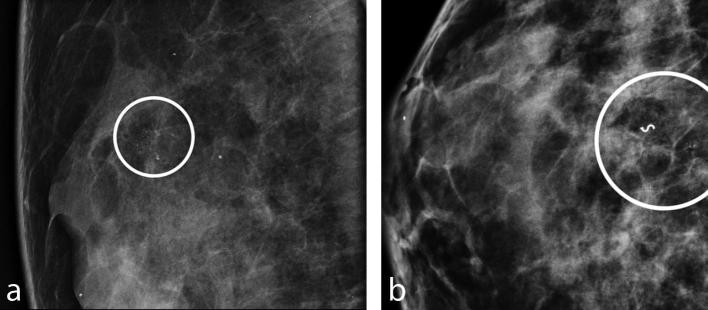
Results: 48 consecutive patients were enrolled in the study, all females, with age range of 39-76 years (mean 53,3 years) and radiological follow-up range of 13-75 months (mean 41.5 months). All the lesions were classified as BI-RADS 4b. The diameter range of the group of calcifications was 3-10 mm (mean 5, 6 mm). In each patient, 7 to 15 samples (mean 11) were obtained. Among all the patients, there was only one case (2%) of new microcalcifications, developed in the same breast, 26 months after and 8 mm from the site of previous VAB, and interpreted as ADH at surgical excision. All the checks of the other patients were negative.
Conclusion: Even with a limited follow-up, we found a malignancy rate lower than 2%, through a defined population. Further studies with bigger number of patients and extended follow-up are needed to reinforce this hypothesis. Advances in knowledge: Surgical excision may not be necessary in patients with VAB diagnosis of isolated FEA, without residual microcalcifications post-procedure and considered concordant with the mammographic presentation, considering the low rate of malignancy at subsequent follow-ups.
Figures

References
-
- Schnitt SJ, Vincent-Salomon A. Columnar cell lesions of the breast. Adv Anat Pathol 2003; 10: 113–24. - PubMed
-
- Azzopardi J. G, Ahmed A, Millis R. R. Problems in breast pathology. Philadelphia: WB Saunders; 1979. - PubMed
-
- Tavassoli F, Millis R, Boecker W. Pathology of the breast. Standford, CT: Appleton Lange; 2003. 60–76.
-
- Perry N, Broeders M, de Wolf C, Törnberg S, Holland R, von Karsa L. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition—summary document. Ann Oncol 2008; 19: 614–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
