

The cost and cost-effectiveness of rapid testing strategies for yaws diagnosis and surveillance
- PMID: 29073145
- PMCID: PMC5658197
- DOI: 10.1371/journal.pntd.0005985
The cost and cost-effectiveness of rapid testing strategies for yaws diagnosis and surveillance
Abstract
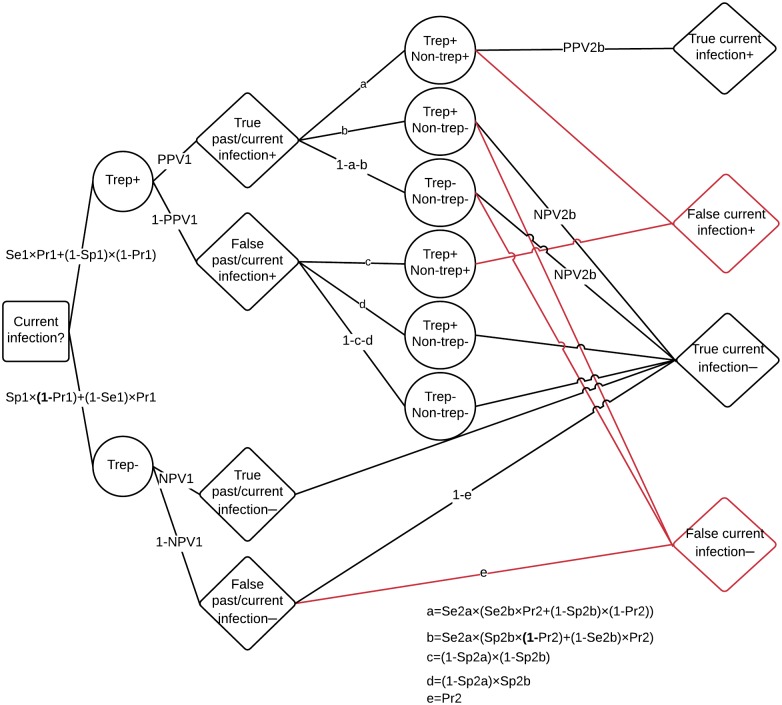
Background: Yaws is a non-venereal treponemal infection caused by Treponema pallidum subspecies pertenue. The disease is targeted by WHO for eradication by 2020. Rapid diagnostic tests (RDTs) are envisaged for confirmation of clinical cases during treatment campaigns and for certification of the interruption of transmission. Yaws testing requires both treponemal (trep) and non-treponemal (non-trep) assays for diagnosis of current infection. We evaluate a sequential testing strategy (using a treponemal RDT before a trep/non-trep RDT) in terms of cost and cost-effectiveness, relative to a single-assay combined testing strategy (using the trep/non-trep RDT alone), for two use cases: individual diagnosis and community surveillance.
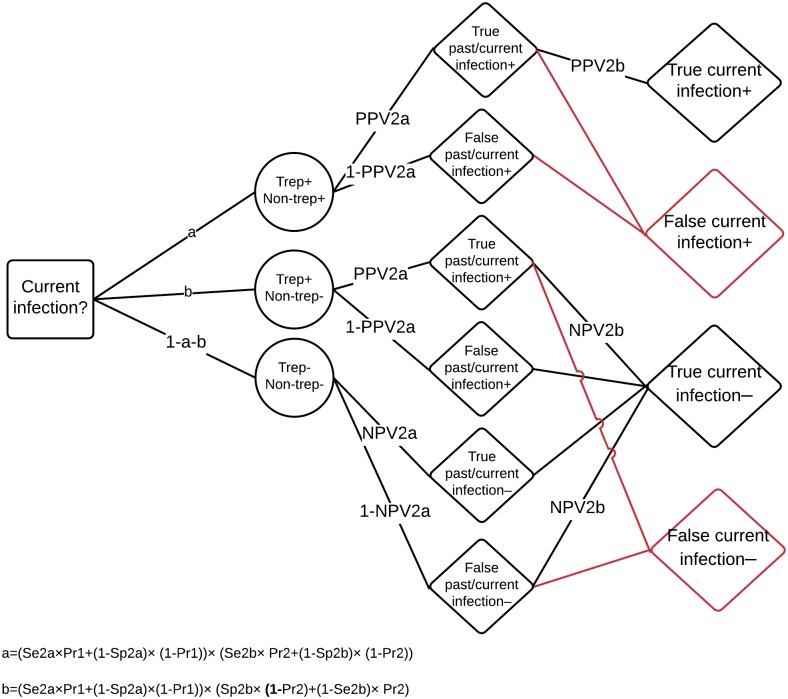
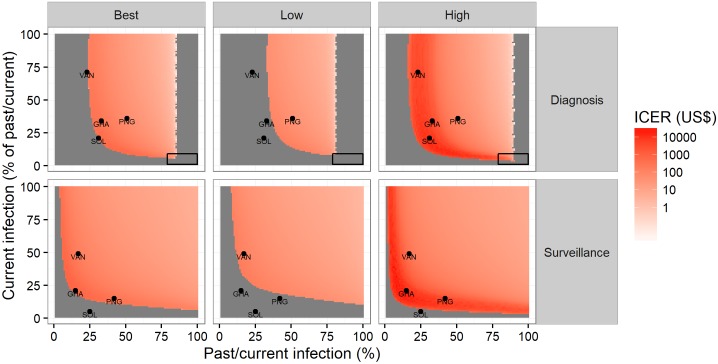
Methods: We use cohort decision analysis to examine the diagnostic and cost outcomes. We estimate cost and cost-effectiveness of the alternative testing strategies at different levels of prevalence of past/current infection and current infection under each use case. We take the perspective of the global yaws eradication programme. We calculate the total number of correct diagnoses for each strategy over a range of plausible prevalences. We employ probabilistic sensitivity analysis (PSA) to account for uncertainty and report 95% intervals.
Results: At current prices of the treponemal and trep/non-trep RDTs, the sequential strategy is cost-saving for individual diagnosis at prevalence of past/current infection less than 85% (81-90); it is cost-saving for surveillance at less than 100%. The threshold price of the trep/non-trep RDT (below which the sequential strategy would no longer be cost-saving) is US$ 1.08 (1.02-1.14) for individual diagnosis at high prevalence of past/current infection (51%) and US$ 0.54 (0.52-0.56) for community surveillance at low prevalence (15%).
Discussion: We find that the sequential strategy is cost-saving for both diagnosis and surveillance in most relevant settings. In the absence of evidence assessing relative performance (sensitivity and specificity), cost-effectiveness is uncertain. However, the conditions under which the combined test only strategy might be more cost-effective than the sequential strategy are limited. A cheaper trep/non-trep RDT is needed, costing no more than US$ 0.50-1.00, depending on the use case. Our results will help enhance the cost-effectiveness of yaws programmes in the 13 countries known to be currently endemic. It will also inform efforts in the much larger group of 71 countries with a history of yaws, many of which will have to undertake surveillance to confirm the interruption of transmission.
Conflict of interest statement
The authors have declared that no competing interests exist. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated. It is not in WHO’s mandate to issue any approvals, certificates or licenses for diagnostics. This responsibility lies with the regulatory authority of each country. Furthermore, WHO does not, as a matter of policy, endorse any specific commercial product over others.
Figures


References
-
- Asiedu K, Fitzpatrick C, Jannin J. Eradication of yaws: historical efforts and achieving WHO’s 2020 target. PLoS Negl Trop Dis. 2014;8: e3016 doi: 10.1371/journal.pntd.0003016 - DOI - PMC - PubMed
-
- Cejkova D, Zobanikova M, Chen L, Pospisilova P, Strouhal M, Qin X, et al. Whole genome sequences of three Treponema pallidum ssp. pertenue strains: yaws and syphilis treponemes differ in less than 0.2% of the genome sequence. PLoS Negl Trop Dis. 2012;6: e1471 doi: 10.1371/journal.pntd.0001471 - DOI - PMC - PubMed
-
- Giacani L, Lukehart SA. The endemic treponematoses. Clin Microbiol Rev. 2014;27: 89–115. doi: 10.1128/CMR.00070-13 - DOI - PMC - PubMed
-
- Ayove T, Houniei W, Wangnapi R, Bieb SV, Kazadi W, Luke LN, et al. Sensitivity and specificity of a rapid point-of-care test for active yaws: a comparative study. Lancet Glob Health. 2014;2: e415–e421. doi: 10.1016/S2214-109X(14)70231-1 - DOI - PubMed
-
- Marks M, Yin Y-P, Chen X-S, Castro A, Causer L, Guy R, et al. Metaanalysis of the Performance of a Combined Treponemal and Nontreponemal Rapid Diagnostic Test for Syphilis and Yaws. Clin Infect Dis Off Publ Infect Dis Soc Am. 2016; doi: 10.1093/cid/ciw348 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
