

The effects of rhythm control strategies versus rate control strategies for atrial fibrillation and atrial flutter: A systematic review with meta-analysis and Trial Sequential Analysis
- PMID: 29073191
- PMCID: PMC5658096
- DOI: 10.1371/journal.pone.0186856
The effects of rhythm control strategies versus rate control strategies for atrial fibrillation and atrial flutter: A systematic review with meta-analysis and Trial Sequential Analysis
Abstract
Background: Atrial fibrillation and atrial flutter may be managed by either a rhythm control strategy or a rate control strategy but the evidence on the clinical effects of these two intervention strategies is unclear. Our objective was to assess the beneficial and harmful effects of rhythm control strategies versus rate control strategies for atrial fibrillation and atrial flutter.
Methods: We searched CENTRAL, MEDLINE, Embase, LILACS, Web of Science, BIOSIS, Google Scholar, clinicaltrials.gov, TRIP, EU-CTR, Chi-CTR, and ICTRP for eligible trials comparing any rhythm control strategy with any rate control strategy in patients with atrial fibrillation or atrial flutter published before November 2016. Our primary outcomes were all-cause mortality, serious adverse events, and quality of life. Our secondary outcomes were stroke and ejection fraction. We performed both random-effects and fixed-effect meta-analysis and chose the most conservative result as our primary result. We used Trial Sequential Analysis (TSA) to control for random errors. Statistical heterogeneity was assessed by visual inspection of forest plots and by calculating inconsistency (I2) for traditional meta-analyses and diversity (D2) for TSA. Sensitivity analyses and subgroup analyses were conducted to explore the reasons for substantial statistical heterogeneity. We assessed the risk of publication bias in meta-analyses consisting of 10 trials or more with tests for funnel plot asymmetry. We used GRADE to assess the quality of the body of evidence.
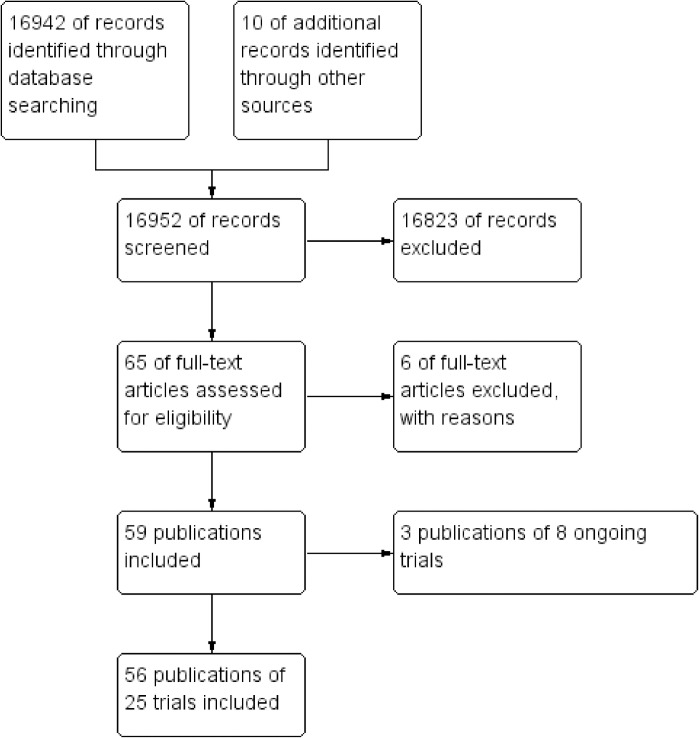
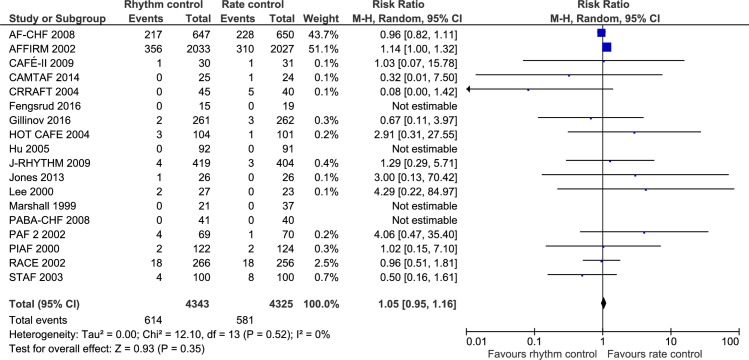
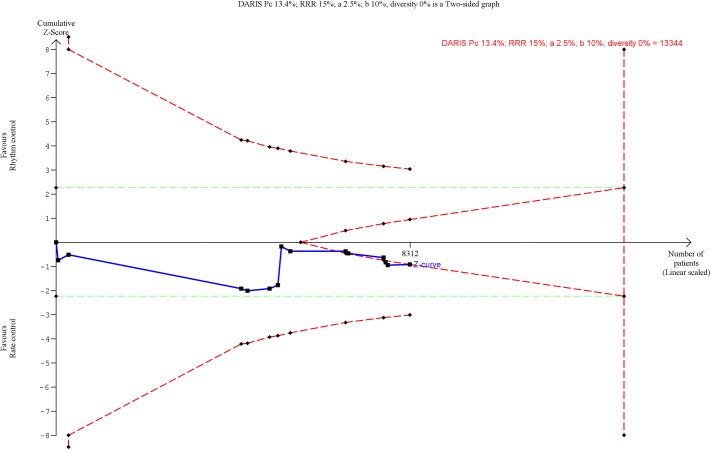
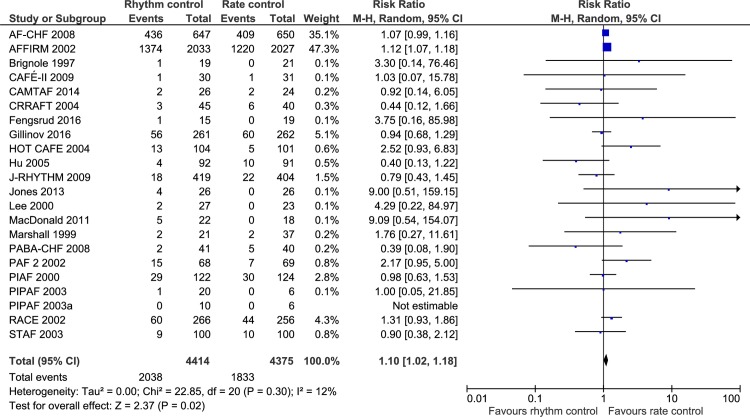
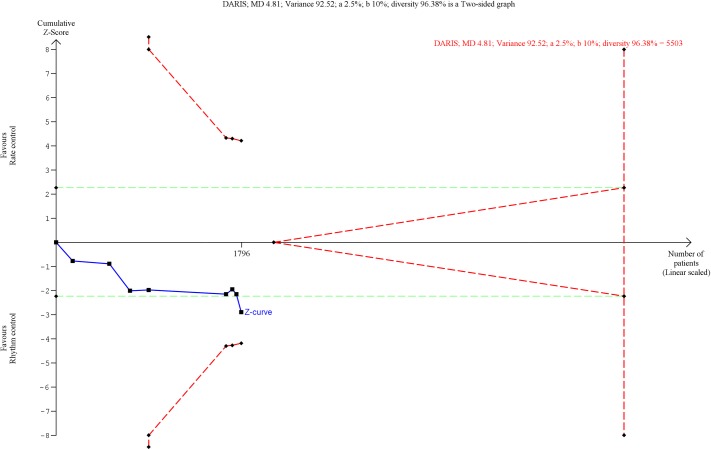
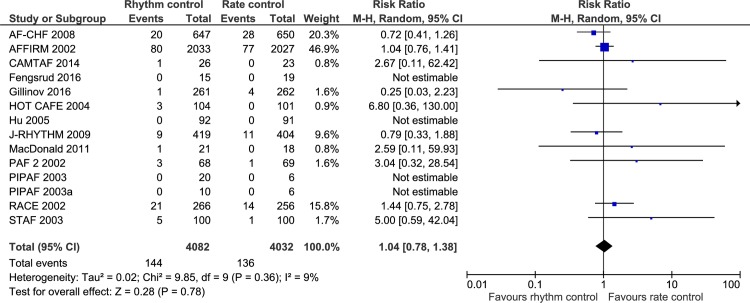
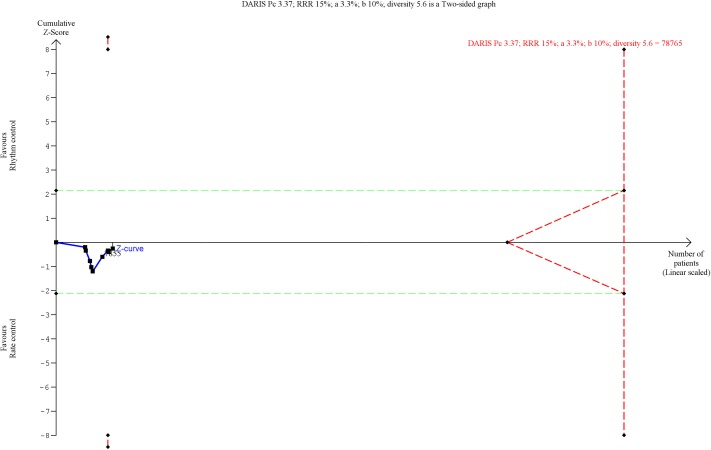
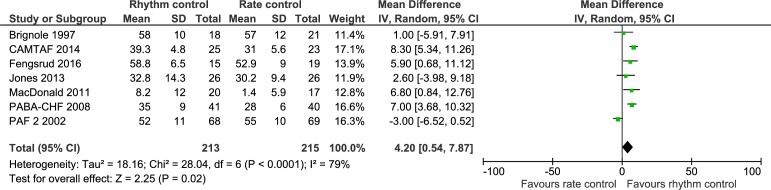
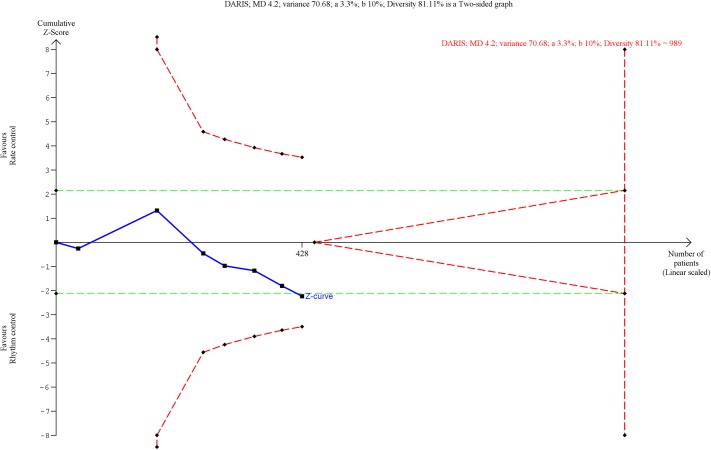
Results: 25 randomized clinical trials (n = 9354 participants) were included, all of which were at high risk of bias. Meta-analysis showed that rhythm control strategies versus rate control strategies significantly increased the risk of a serious adverse event (risk ratio (RR), 1.10; 95% confidence interval (CI), 1.02 to 1.18; P = 0.02; I2 = 12% (95% CI 0.00 to 0.32); 21 trials), but TSA did not confirm this result (TSA-adjusted CI 0.99 to 1.22). The increased risk of a serious adverse event did not seem to be caused by any single component of the composite outcome. Meta-analysis showed that rhythm control strategies versus rate control strategies were associated with better SF-36 physical component score (mean difference (MD), 6.93 points; 95% CI, 2.25 to 11.61; P = 0.004; I2 = 95% (95% CI 0.94 to 0.96); 8 trials) and ejection fraction (MD, 4.20%; 95% CI, 0.54 to 7.87; P = 0.02; I2 = 79% (95% CI 0.69 to 0.85); 7 trials), but TSA did not confirm these results. Both meta-analysis and TSA showed no significant differences on all-cause mortality, SF-36 mental component score, Minnesota Living with Heart Failure Questionnaire, and stroke.
Conclusions: Rhythm control strategies compared with rate control strategies seem to significantly increase the risk of a serious adverse event in patients with atrial fibrillation. Based on current evidence, it seems that most patients with atrial fibrillation should be treated with a rate control strategy unless there are specific reasons (e.g., patients with unbearable symptoms due to atrial fibrillation or patients who are hemodynamically unstable due to atrial fibrillation) justifying a rhythm control strategy. More randomized trials at low risk of bias and low risk of random errors are needed.
Trial registration: PROSPERO CRD42016051433.
Conflict of interest statement
Figures


References
-
- Pistoia F, Sacco S, Tiseo C, Degan D, Ornello R, Carolei A. The epidemiology of atrial fibrillation and stroke. Cardiology Clinics. 2016;34(2):255–68. doi: 10.1016/j.ccl.2015.12.002 - DOI - PubMed
-
- Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Europace. 2012;14(10):1385–413. doi: 10.1093/europace/eus305 - DOI - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. American Journal of Medicine. 2002;113(5):359–64. - PubMed
-
- Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98(10):946–52. - PubMed
-
- Rahman F, Wang N, Yin X, Ellinor PT, Lubitz SA, LeLorier PA, et al. Atrial flutter: clinical risk factors and adverse outcomes in the Framingham Heart Study. Heart Rhythm. 2016;13(1):233–40. doi: 10.1016/j.hrthm.2015.07.031 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
