

The SDM 3 Circle Model: A Literature Synthesis and Adaptation for Shared Decision Making in the Hospital
- PMID: 29073314
- PMCID: PMC5709161
- DOI: 10.12788/jhm.2865
The SDM 3 Circle Model: A Literature Synthesis and Adaptation for Shared Decision Making in the Hospital
Abstract
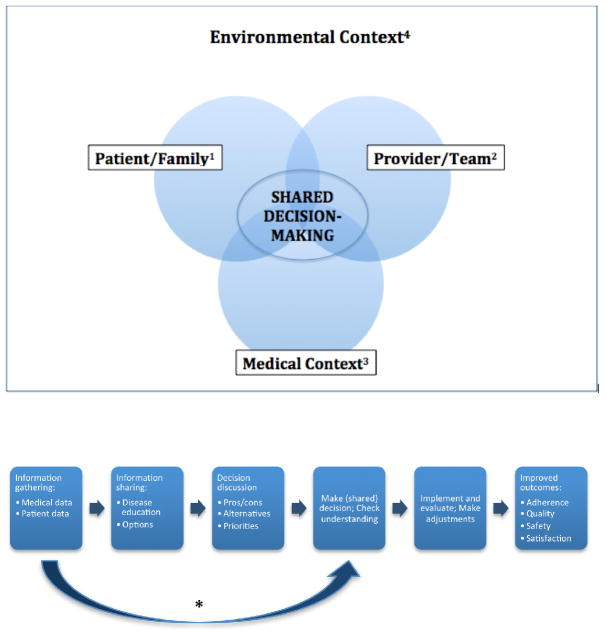
Patient engagement through shared decision-making (SDM) is increasingly seen as a key component for patient safety, patient satisfaction, and quality of care. Current SDM models do not adequately account for medical and environmental contexts, which may influence medical decisions in the hospital. We identified leading SDM models and reviews to inductively construct a novel SDM model appropriate for the inpatient setting. A team of medicine and pediatric hospitalists reviewed the literature to integrate core SDM concepts and processes and iteratively constructed a synthesized draft model. We then solicited broad SDM expert feedback on the draft model for validation and further refinement. The SDM 3 Circle Model identifies 3 core categories of variables that dynamically interact within an "environmental frame." The resulting Venn diagram includes overlapping circles for (1) patient/family, (2) provider/team, and (3) medical context. The environmental frame includes all external, contextual factors that may influence any of the 3 circles. Existing multistep SDM process models were then rearticulated and contextualized to illustrate how a shared decision might be made. The SDM 3 Circle Model accounts for important environmental and contextual characteristics that vary across settings. The visual emphasis generated by each "circle" and by the environmental frame direct attention to often overlooked interactive forces and has the potential to more precisely define, promote, and improve SDM. This model provides a framework to develop interventions to improve quality and patient safety through SDM and patient engagement for hospitalists.
© 2017 Society of Hospital Medicine.
Figures
References
-
- Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med 1982. 1999;49(5):651–661. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
