

Gut Microbiota Perturbations in Reactive Arthritis and Postinfectious Spondyloarthritis
- PMID: 29073348
- PMCID: PMC5788722
- DOI: 10.1002/art.40359
Gut Microbiota Perturbations in Reactive Arthritis and Postinfectious Spondyloarthritis
Abstract
Objective: Reactive arthritis (ReA) is an inflammatory disorder occurring several weeks after gastrointestinal or genitourinary tract infections. HLA-B27 positivity is considered a risk factor, although it is not necessarily predictive of disease incidence. Among nongenetic factors, the intestinal microbiome may play a role in disease susceptibility. The objective of this study was to characterize the gut microbiota and host gene interactions in ReA and postinfectious spondyloarthritis.
Methods: Adult subjects with peripheral spondyloarthritis and control subjects with preceding infections who did not develop arthritis were prospectively recruited from a geographic region with a high prevalence of ReA. Clinical variables, HLA status, and 16S ribosomal RNA gene sequencing of intestinal microbiota were analyzed.
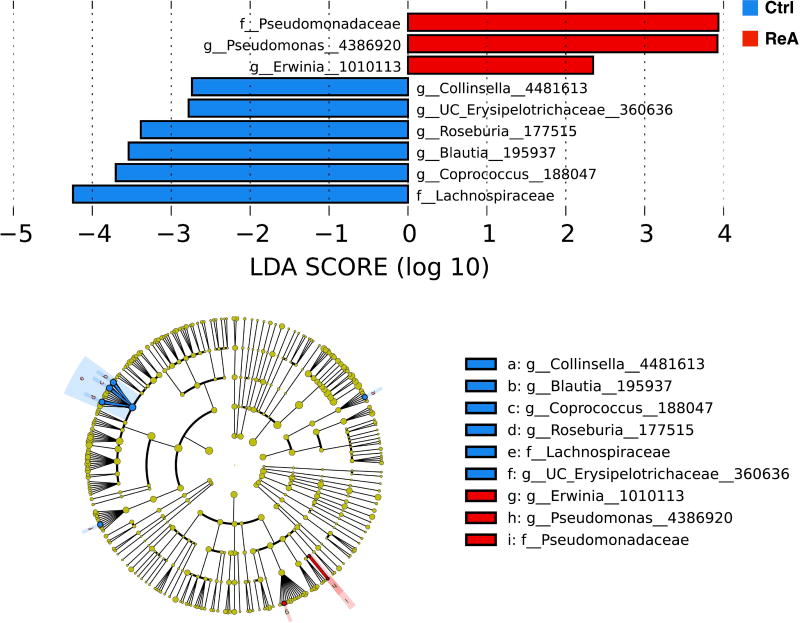
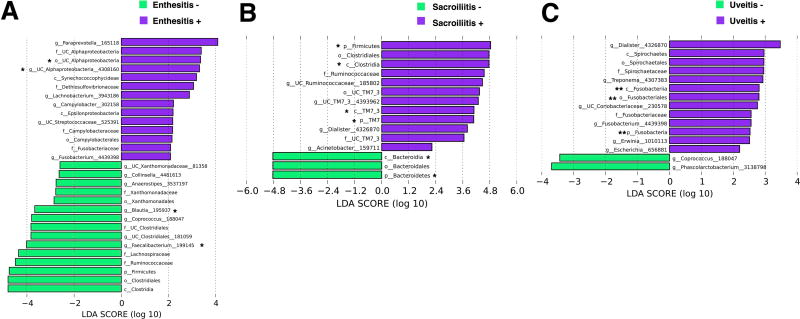
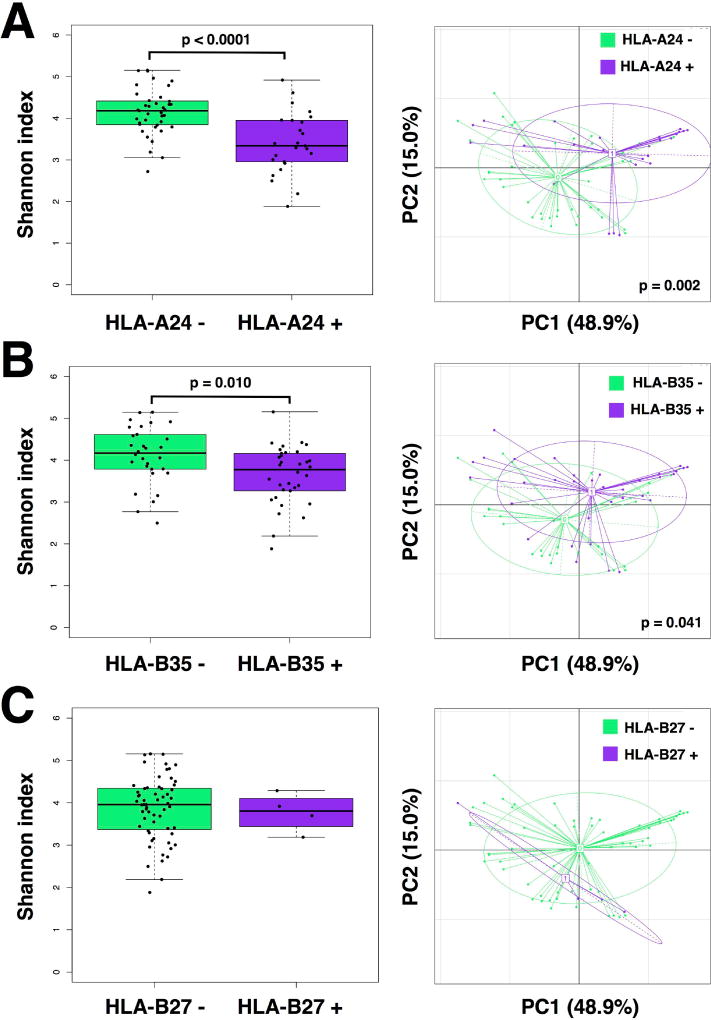
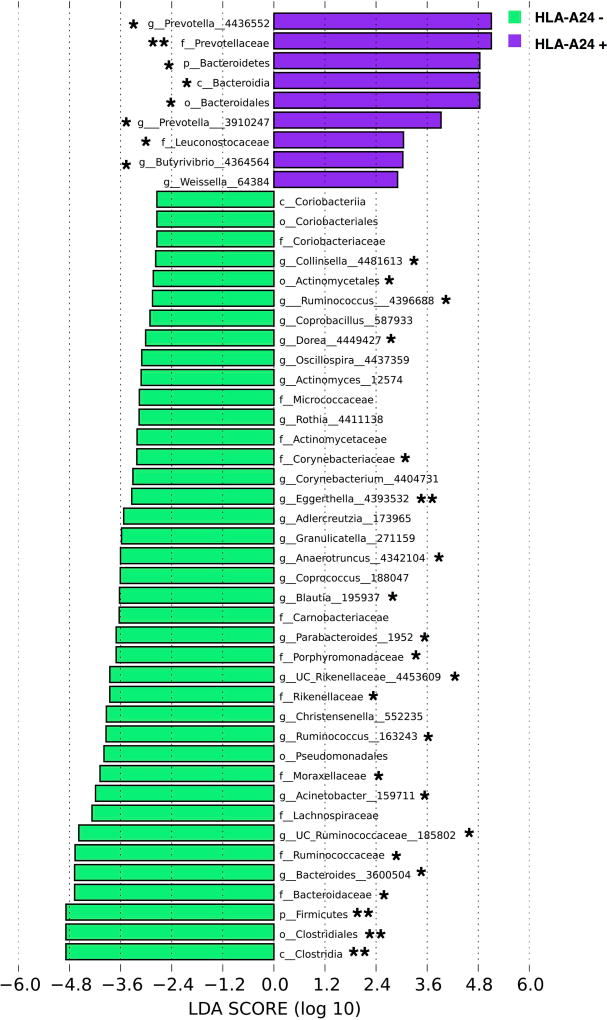
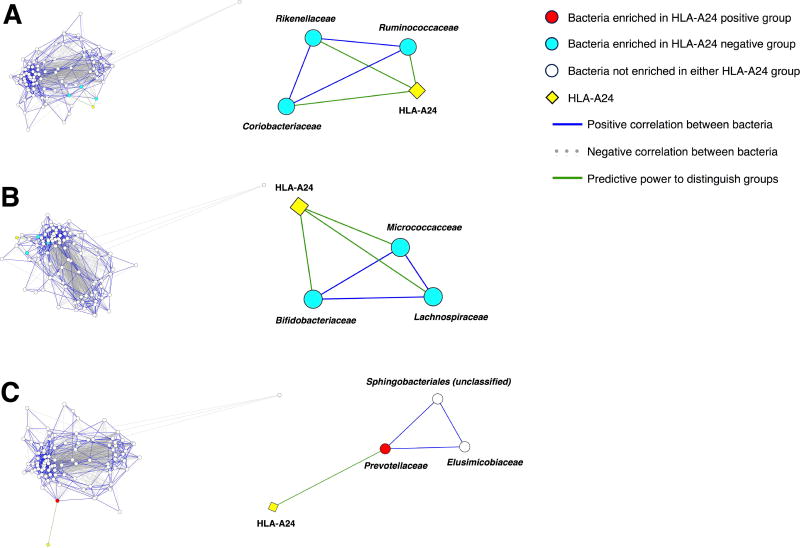
Results: Subjects with ReA showed no significant differences from controls in gut bacterial richness or diversity. However, there was a significantly higher abundance of Erwinia and Pseudomonas and an increased prevalence of typical enteropathogens associated with ReA. Subjects with ultrasound evidence of enthesitis were enriched in Campylobacter, while subjects with uveitis and radiographic sacroiliitis were enriched in Erwinia and unclassified Ruminococcaceae, respectively; both were enriched in Dialister. Host genetics, particularly HLA-A24, were associated with differences in gut microbiota diversity irrespective of disease status. We identified several co-occurring taxa that were also predictive of HLA-A24 status.
Conclusion: This is the first culture-independent study characterizing the gut microbial community in postinfectious arthritis. Although bacterial factors correlated with disease presence and clinical features of ReA, host genetics also appeared to be a major independent driver of intestinal community composition. Understanding of these gut microbiota-host genetic relationships may further clarify the pathogenesis of postinfectious spondyloarthritides.
© 2017, American College of Rheumatology.
Figures
References
-
- Hannu T. Reactive arthritis. Best Pract Res Clin Rheumatol. 2011;25(3):347–57. - PubMed
-
- Schiellerup P, Krogfelt KA, Locht H. A comparison of self-reported joint symptoms following infection with different enteric pathogens: effect of HLA-B27. J Rheumatol. 2008;35(3):480–7. - PubMed
-
- Putterman C, Rubinow A. Reactive arthritis associated with Clostridium difficile pseudomembranous colitis. Semin Arthritis Rheum. 1993;22(6):420–6. - PubMed
-
- Brewerton DA, Caffrey M, Nicholls A, Walters D, Oates JK, James DC. Reiter's disease and HL-A 27. Lancet. 1973;302(7836):996–8. - PubMed
-
- Khan MA. HLA-B27 and its subtypes in world populations. Curr Opin Rheumatol. 1995;7(4):263–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
