

Phenotype and Clinical Outcomes of Titin Cardiomyopathy
- PMID: 29073955
- PMCID: PMC5666113
- DOI: 10.1016/j.jacc.2017.08.063
Phenotype and Clinical Outcomes of Titin Cardiomyopathy
Abstract
Background: Improved understanding of dilated cardiomyopathy (DCM) due to titin truncation (TTNtv) may help guide patient stratification.
Objectives: The purpose of this study was to establish relationships among TTNtv genotype, cardiac phenotype, and outcomes in DCM.
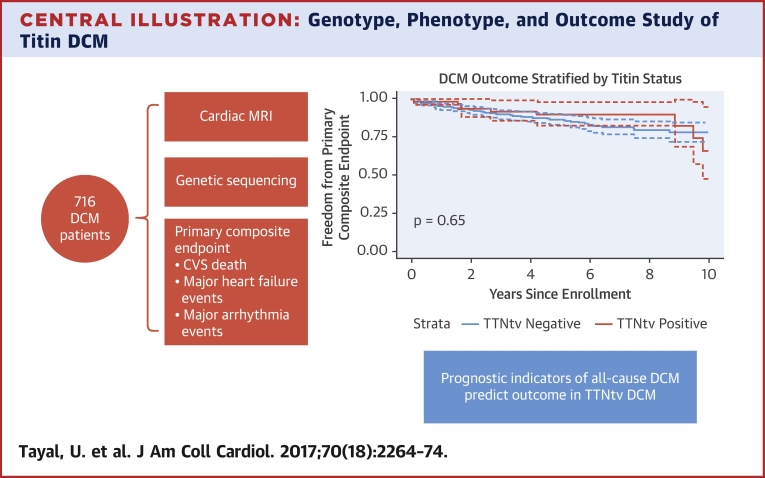
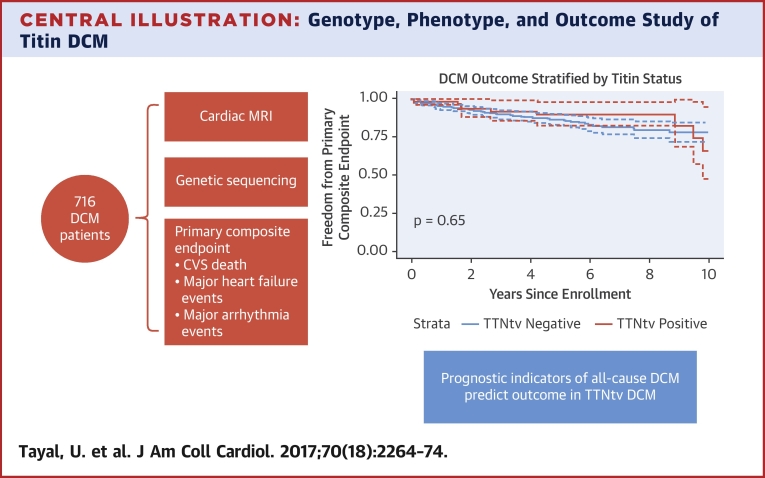
Methods: In this prospective, observational cohort study, DCM patients underwent clinical evaluation, late gadolinium enhancement cardiovascular magnetic resonance, TTN sequencing, and adjudicated follow-up blinded to genotype for the primary composite endpoint of cardiovascular death, and major arrhythmic and major heart failure events.
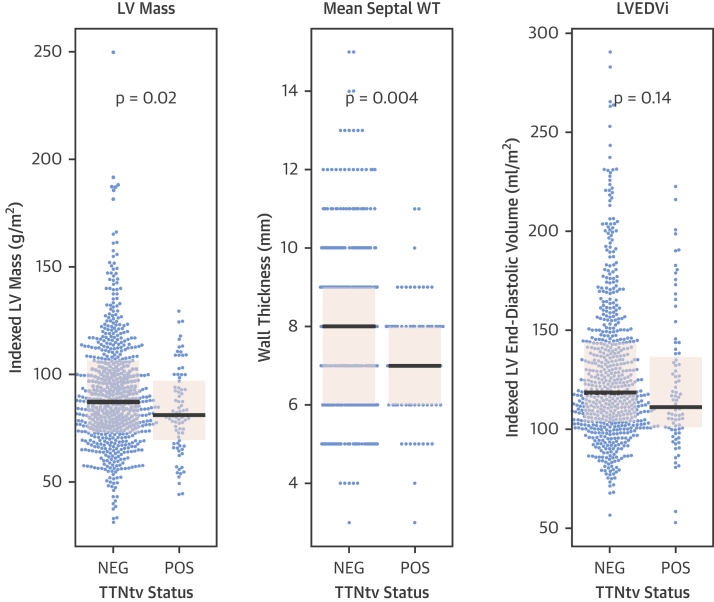
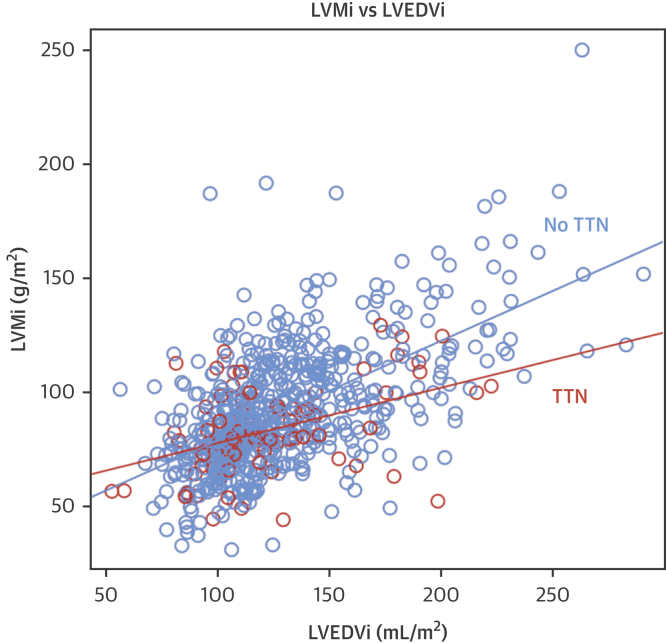
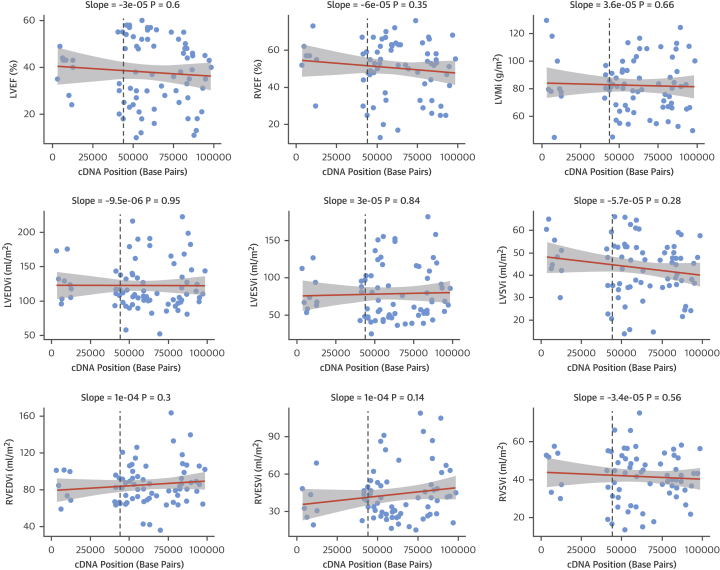
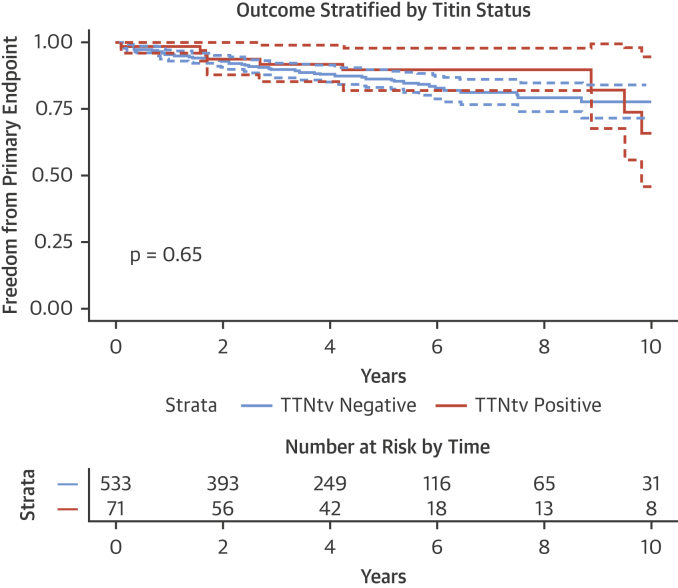
Results: Of 716 subjects recruited (mean age 53.5 ± 14.3 years; 469 men [65.5%]; 577 [80.6%] New York Heart Association function class I/II), 83 (11.6%) had TTNtv. Patients with TTNtv were younger at enrollment (49.0 years vs. 54.1 years; p = 0.002) and had lower indexed left ventricular mass (5.1 g/m2 reduction; padjusted = 0.03) compared with patients without TTNtv. There was no difference in biventricular ejection fraction between TTNtv+/- groups. Overall, 78 of 604 patients (12.9%) met the primary endpoint (median follow-up 3.9 years; interquartile range: 2.0 to 5.8 years), including 9 of 71 patients with TTNtv (12.7%) and 69 of 533 (12.9%) without. There was no difference in the composite primary outcome of cardiovascular death, heart failure, or arrhythmic events, for patients with or without TTNtv (hazard ratio adjusted for primary endpoint: 0.92 [95% confidence interval: 0.45 to 1.87]; p = 0.82).
Conclusions: In this large, prospective, genotype-phenotype study of ambulatory DCM patients, we show that prognostic factors for all-cause DCM also predict outcome in TTNtv DCM, and that TTNtv DCM does not appear to be associated with worse medium-term prognosis.
Keywords: CMR; DCM; genetics; titin.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Should Identifying a Titin Truncating Variant Change the Management of Patients With Dilated Cardiomyopathy?J Am Coll Cardiol. 2017 Oct 31;70(18):2275-2277. doi: 10.1016/j.jacc.2017.09.020. J Am Coll Cardiol. 2017. PMID: 29073956 No abstract available.
References
-
- Hershberger R.E., Hedges D.J., Morales A. Dilated cardiomyopathy: the complexity of a diverse genetic architecture. Nat Rev Cardiol. 2013;10:531–547. - PubMed
-
- Maron B.J., Towbin J.A., Thiene G. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. - PubMed
-
- International Society of Heart and Lung Transplantation Quarterly Report. 2015 edition. Available at: https://www.ishlt.org/registries/quarterlyDataReportStep3.asp?organ=HR&r.... Accessed September 9, 2017.
-
- Kober L., Thune J.J., Nielsen J.C. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med. 2016;375:1221–1230. - PubMed
-
- Gulati A., Jabbour A., Ismail T.F. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. JAMA. 2013;309:896–908. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
