

Improving margin revision: Characterization of tumor bed margins in early oral tongue cancer
- PMID: 29074194
- PMCID: PMC5774620
- DOI: 10.1016/j.oraloncology.2017.10.013
Improving margin revision: Characterization of tumor bed margins in early oral tongue cancer
Abstract
Objectives: To improve margin revision, this study characterizes the number, fragmentation, and orientation of tumor bed margins (TBM) in patients with pT1-2 pN0 squamous cell carcinoma (SCC) of the oral tongue.
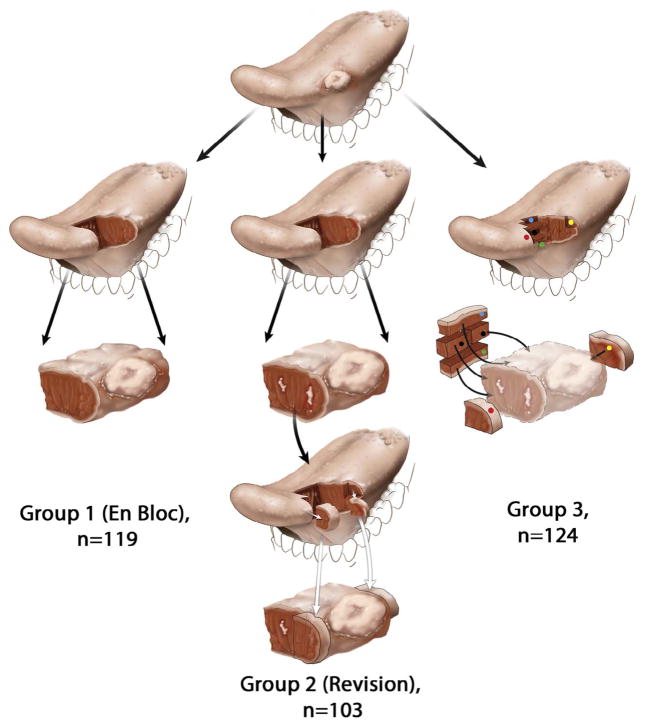
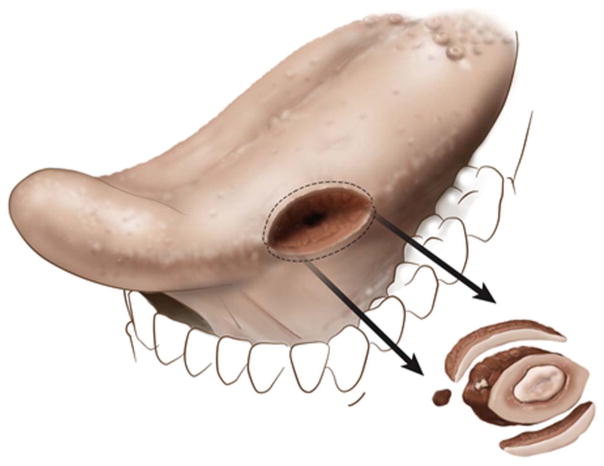
Materials and methods: Pathology reports (n=346) were reviewed. TBM parameters were indexed. In Group 1 patients all margins were obtained from the glossectomy specimen and there were no TBM. In Revision Group/Group 2 (n=103), tumor bed was sampled to revise suboptimal margins identified by examination of the glossectomy specimen. In Group 3 (n=124), TBM were obtained before examination of the glossectomy specimen.
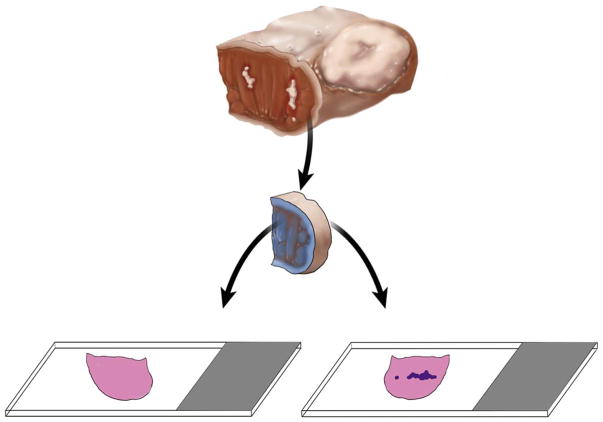
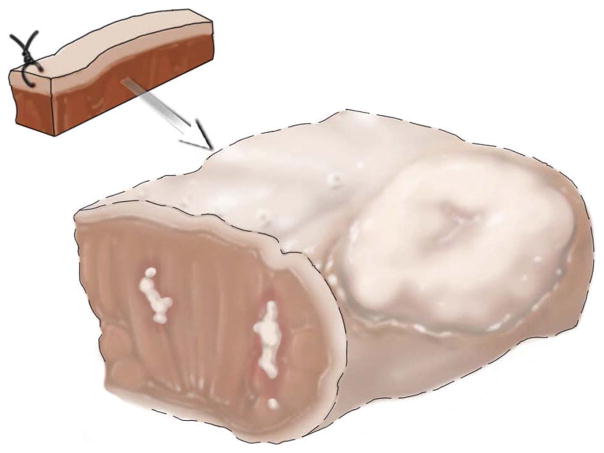
Results and conclusions: Fewer TBMs were obtained per patient in Group 2 compared to Group 3 (57/103, 55% of patients with <3 vs. 117/124, 94%, ≥3 TBMs, respectively). The new margin surface was more frequently indicated in Group 2 compared to Group 3 (59/103, 57%, vs. 19/124, 15%, p<.001). If glossectomy specimen margins are accepted as the reference standard, then the TBM was 15% sensitive in Group 2 (95% confidence interval [CI], 7-29) and 32% sensitive in Group 3 (95% CI, 15-55). TBM fragmentation (23/103, 22% vs. 42/124, 34%) and frozen vs. permanent discrepancies (8/103, 3% vs. 3/124, 2%) were similar between Groups 2 and 3. The new margin surface was not indicated in 6 of 11 cases with discrepant frozen vs. permanent pathology findings, precluding judgment on final margin status. To facilitate the assessment of final margins, TBM should be represented by one tissue fragment with a marked new margin surface.
Keywords: Margin fragmentation; Margin orientation; Oral tongue; Revision; Specimen margin; Squamous cell carcinoma; Tumor bed margin.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
None.
Figures

References
-
- Weinstock YE, Alava I, 3rd, Dierks EJ. Pitfalls in determining head and neck surgical margins. Oral Maxillofac Surg Clin North Am. 2014;26:151–62. - PubMed
-
- Chen AY. Quality initiatives in head and neck cancer. Curr Oncol Rep. 2010;12:109–14. - PubMed
-
- Black C, Marotti J, Zarovnaya E, Paydarfar J. Critical evaluation of frozen section margins in head and neck cancer resections. Cancer. 2006;107:2792–800. - PubMed
-
- Meier JD, Oliver DA, Varvares MA. Surgical margin determination in head and neck oncology: current clinical practice. The results of an International American Head and Neck Society Member Survey. Head Neck. 2005;27:952–8. - PubMed
-
- Hinni ML, Ferlito A, Brandwein-Gensler MS, Takes RP, Silver CE, Westra WH, et al. Surgical margins in head and neck cancer: a contemporary review. Head Neck. 2013;35:1362–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
