

The incidence of congenital hypothyroidism (CH) in Guangxi, China and the predictors of permanent and transient CH
- PMID: 29074613
- PMCID: PMC5704446
- DOI: 10.1530/EC-17-0289
The incidence of congenital hypothyroidism (CH) in Guangxi, China and the predictors of permanent and transient CH
Abstract
Background: The incidence of congenital hypothyroidism (CH) differs significantly among different ethnicities and regions, and early differentiation of transient CH is important to avoid unnecessary prolonged treatment with L-T4.
Objective: To investigate the incidence of CH based on the newborn screening program in Guangxi Zhuang Autonomous Region, China, and to analyze the predictors that might allow for an early differentiation between permanent (P) and transient (T) CH.
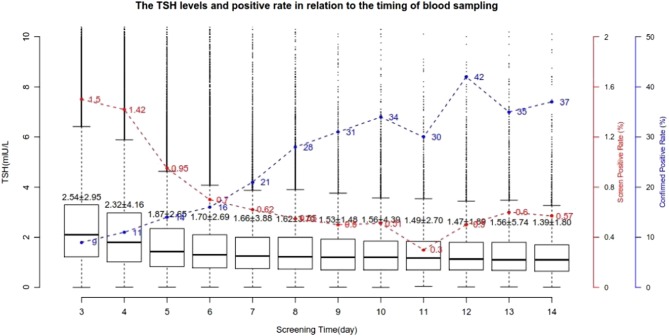
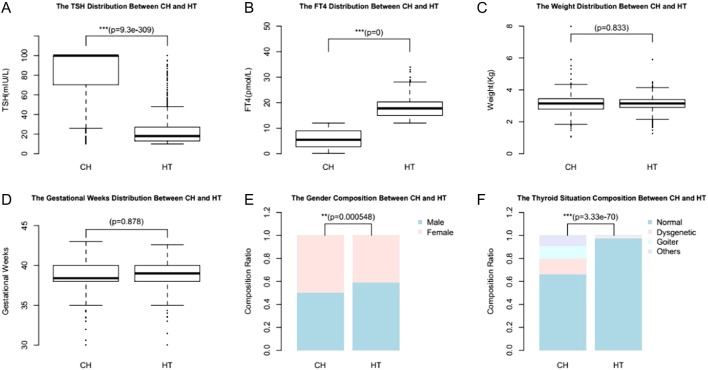
Design and methods: Data from newborn screening program over a seven-year period (January 2009 to January 2016) at Guangxi Maternal and Child Health Hospital are analyzed. Blood samples were collected on filter paper between 3 and 7 days after birth, and TSH level was measured by time-resolved fluorescence assay. Individuals with increased TSH (TSH ≥ 8 IU/L) levels detected by newborn screening were recalled for further evaluation. Serum TSH, FT3 and FT4 were determined by electrochemiluminescence assay using venous blood samples. Diagnosis of CH is based on elevated TSH levels (>10 IU/L) and decreased FT4 levels (<12 pmol/L). Patients with elevated TSH levels and normal FT4 levels were diagnosed as hyperthyrotropinemia. Permanent or transient CH was determined by using the results of thyroid function tests after temporary withdrawal of L-T4 therapy at approximately 2-3 years of age.
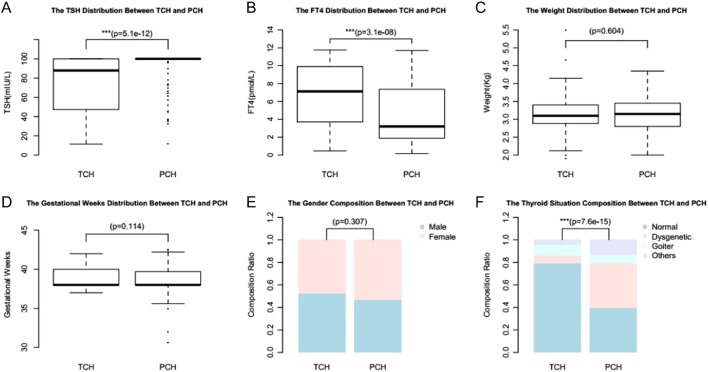
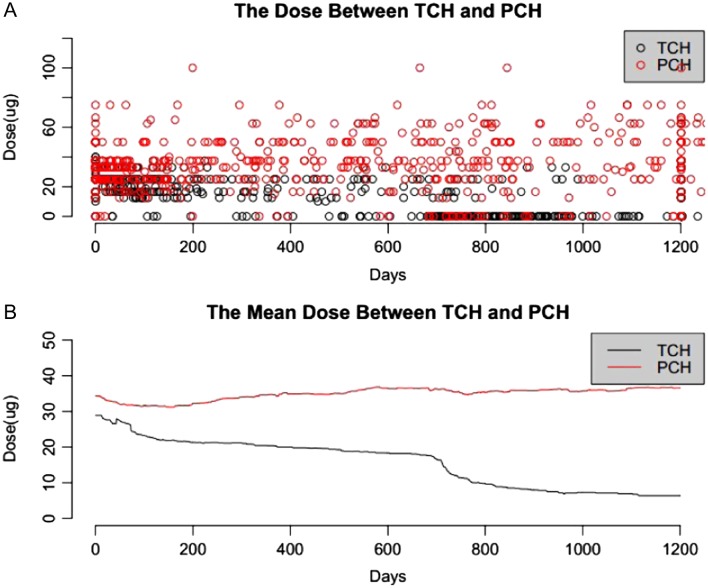
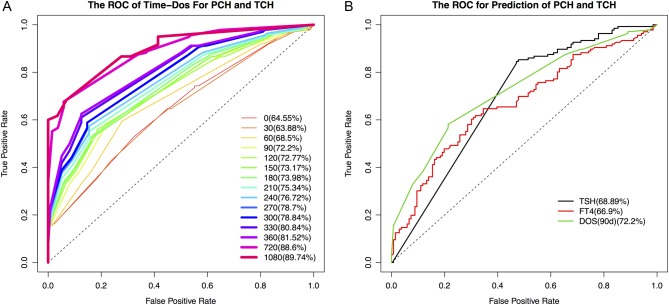
Results: Among 1,238,340 infants in the newborn screening program, 14,443 individuals were recalled for reevaluation (re-call rate 1.18%), 911 and 731 individuals were subsequently determined to have hyperthyrotropinemia and CH respectively; thus, a prevalence of 1:1359 and 1:1694 for hyperthyrotropinemia and CH. Of the 731 patients with CH, 161 patients were diagnosed with permanent CH (PCH), and 159 patients were diagnosed with transient CH (TCH), the other 411 patients are too young to determine their subtypes. Patients with PCH required an increasing dose of L-T4 during the first few years, whereas patients with TCH required a decreased dose of L-T4. The TSH levels at diagnosis and the dose of L-T4 used were significantly higher in PCH cases than in transient cases. The FT4 levels at diagnosis were significantly lower in PCH cases than in TCH cases. The TSH levels at diagnosis, FT4 levels at diagnosis and L-T4 doses at 90 days were evaluated as predictors for differentiating PCH and TCH, and their accuracy at their respective optimal cutoffs were determined to be 60.6%, 66.7% and 93.9%, respectively.
Conclusions: The CH incidence in Guangxi Zhuang Autonomous Region is slightly higher (1:1694) compared to the worldwide levels (1/2000-1/4000). The PCH and TCH ratio is close to 1; thus, the estimated PCH incidence is 1/3388, which is similar to reported worldwide average incidence (1/3000). The L-T4 dose required at 90 days (>30 μg/day) has the highest predictive value for PCH. Earlier differentiation of PCH and TCH helps to determine appropriate treatment course.
Keywords: China; Guangxi; L-T4 dose; congenital hypothyroidism; predictor; prevalence.
© 2017 The authors.
Figures
References
-
- Hermanns P, Grasberger H, Cohen R, Freiberg C, Dorr HG, Refetoff S, Pohlenz J. Two cases of thyroid dysgenesis caused by different novel PAX8 mutations in the DNA-binding region: in vitro studies reveal different pathogenic mechanisms. Thyroid 2013. 23 791–796. ( 10.1089/thy.2012.0141) - DOI - PMC - PubMed
-
- Kocova M, Anastasovska V, Sukarova-Angelovska E, Tanaskoska M, Taseva E. Clinical practice: experience with newborn screening for congenital hypothyroidism in the Republic of Macedonia – a multiethnic country. European Journal of Pediatrics 2015. 174 443–448. ( 10.1007/s00431-014-2413-4) - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
