

Randomized Clinical Trial of Sevelamer Carbonate on Serum Klotho and Fibroblast Growth Factor 23 in CKD
- PMID: 29074818
- PMCID: PMC5718266
- DOI: 10.2215/CJN.03030317
Randomized Clinical Trial of Sevelamer Carbonate on Serum Klotho and Fibroblast Growth Factor 23 in CKD
Abstract
Background and objectives: Epidemiologic studies suggest that higher serum phosphaturic hormone fibroblast growth factor 23 levels are associated with increase morbidity and mortality. The aim of the FGF23 Reduction Efficacy of a New Phosphate Binder in CKD Trial was to evaluate the effect of sevelamer carbonate on serum C-terminal fibroblast growth factor 23 levels in normophosphatemic patients with CKD stage 3b/4.
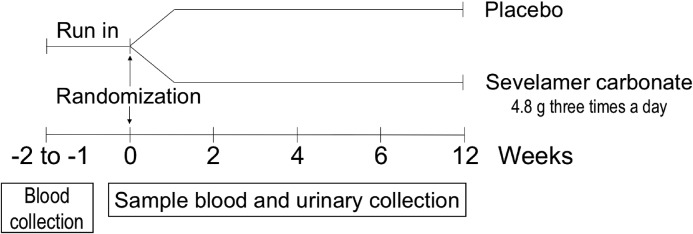
Design, setting, participants, & measurements: Patients with CKD, eGFR between 45 and 15 ml/min per 1.73 m2, fasting serum phosphate concentration >3.1 mg/dl, and serum C-terminal fibroblast growth factor 23 >80 relative units/ml were included in our double-blind, placebo-controlled, randomized multicenter study. All patients received 100,000 IU cholecalciferol at time of randomization. Participants received either placebo or sevelamer carbonate 4.8 g daily during a 12-week period. Biologic parameters, including serum C-terminal fibroblast growth factor 23, intact fibroblast growth factor 23, and α-klotho, were evaluated at baseline and 12 weeks after inclusion.
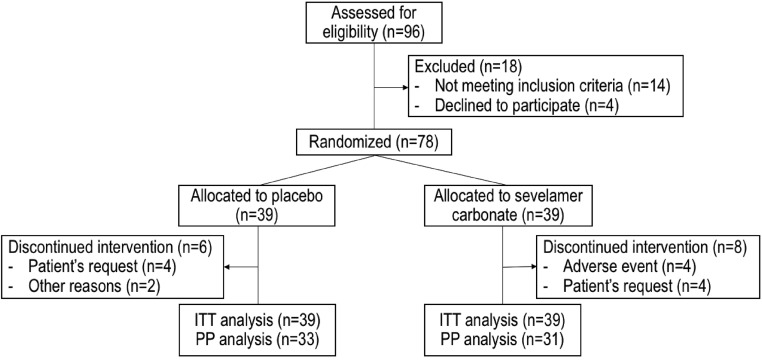
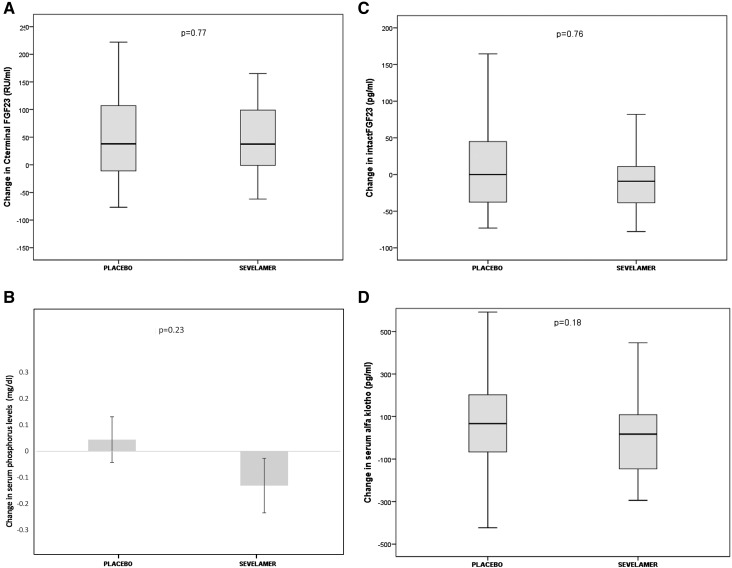
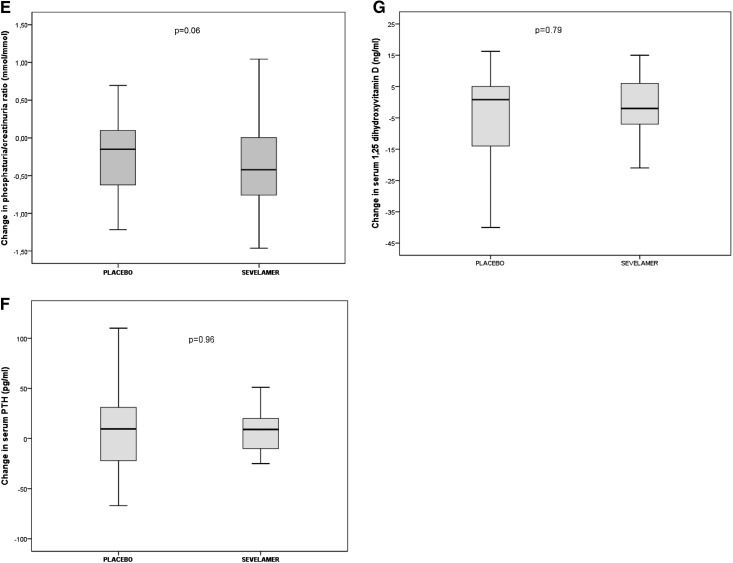
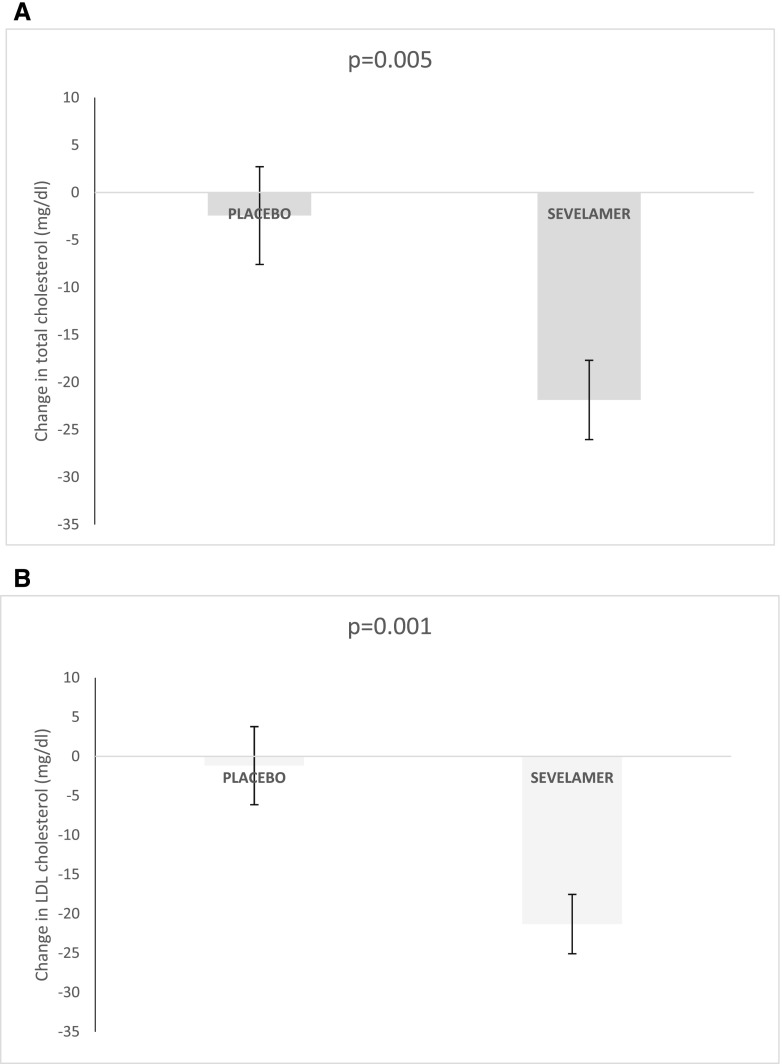
Results: Of 96 screened patients, 78 (mean±SD age: 63±13 years old; 70% men; mean eGFR: 27±9 ml/min per 1.73 m2) met the inclusion criteria. At baseline, mean eGFR was 27±9 ml/min per 1.73 m2, mean serum phosphate level was 3.8±0.5 mg/dl, and median (interquartile range) serum C-terminal fibroblast growth factor 23 level was 157 (120-241) relative units/ml. After 12 weeks of treatment, urinary phosphate-to-creatinine ratio fell significantly in the sevelamer group. The sevelamer and placebo groups did not differ significantly in terms of median change in serum C-terminal fibroblast growth factor 23 levels: the median (interquartile range) change was 38 (-13-114) relative units/ml in the placebo group and 37 (-1-101) relative units/ml in the sevelamer group (P=0.77). There was no significant difference in serum intact fibroblast growth factor 23, α-klotho, or phosphate levels changes between the two groups. Serum total and LDL cholesterol levels fell significantly in the sevelamer group.
Conclusions: In our double-blind, placebo-controlled, randomized study performed in normophosphatemic patients with CKD, a 12-week course of sevelamer carbonate significantly reduced phosphaturia without changing serum phosphorus but did not significantly modify serum C-terminal fibroblast growth factor 23 and intact fibroblast growth factor 23 or α-klotho levels.
Keywords: Cholecalciferol; Cholesterol, LDL; Double-Blind Method; Epidemiologic Studies; FGF23; Fasting; Fibroblast Growth Factors; Hypophosphatemia, Familial; KLOTHO; Phosphates; Phosphorus; Random Allocation; Renal Insufficiency, Chronic; chronic kidney disease; creatinine; fibroblast; fibroblast growth factor 23; glomerular filtration rate; mineral metabolism; phosphate binders; randomized controlled trials; sevelamer.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Continued Search for Therapies to Favorably Modify Phosphate and FGF23 Levels in CKD.Clin J Am Soc Nephrol. 2017 Dec 7;12(12):1911-1913. doi: 10.2215/CJN.11011017. Epub 2017 Oct 26. Clin J Am Soc Nephrol. 2017. PMID: 29074819 Free PMC article. No abstract available.
References
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJL, Mann JF, Matsushita K, Wen CP: Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 382: 339–352, 2013 - PubMed
-
- Palmer SC, Hayen A, Macaskill P, Pellegrini F, Craig JC, Elder GJ, Strippoli GFM: Serum levels of phosphorus, parathyroid hormone, and calcium and risks of death and cardiovascular disease in individuals with chronic kidney disease: A systematic review and meta-analysis. JAMA 305: 1119–1127, 2011 - PubMed
-
- Isakova T, Wahl P, Vargas GS, Gutiérrez OM, Scialla J, Xie H, Appleby D, Nessel L, Bellovich K, Chen J, Hamm L, Gadegbeku C, Horwitz E, Townsend RR, Anderson CAM, Lash JP, Hsu C-Y, Leonard MB, Wolf M: Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int 79: 1370–1378, 2011 - PMC - PubMed
-
- Fliser D, Kollerits B, Neyer U, Ankerst DP, Lhotta K, Lingenhel A, Ritz E, Kronenberg F, Kuen E, König P, Kraatz G, Mann JF, Müller GA, Köhler H, Riegler P; MMKD Study Group : Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: The Mild to Moderate Kidney Disease (MMKD) study. J Am Soc Nephrol 18: 2600–2608, 2007 - PubMed
-
- Desjardins L, Liabeuf S, Renard C, Lenglet A, Lemke H-D, Choukroun G, Drueke TB, Massy ZA; European Uremic Toxin (EUTox) Work Group : FGF23 is independently associated with vascular calcification but not bone mineral density in patients at various CKD stages. Osteoporos Int 23: 2017–2025, 2012 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
