

Motor recovery after activity-based training with spinal cord epidural stimulation in a chronic motor complete paraplegic
- PMID: 29074997
- PMCID: PMC5658385
- DOI: 10.1038/s41598-017-14003-w
Motor recovery after activity-based training with spinal cord epidural stimulation in a chronic motor complete paraplegic
Abstract
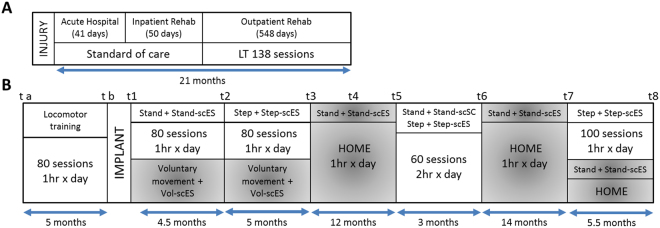
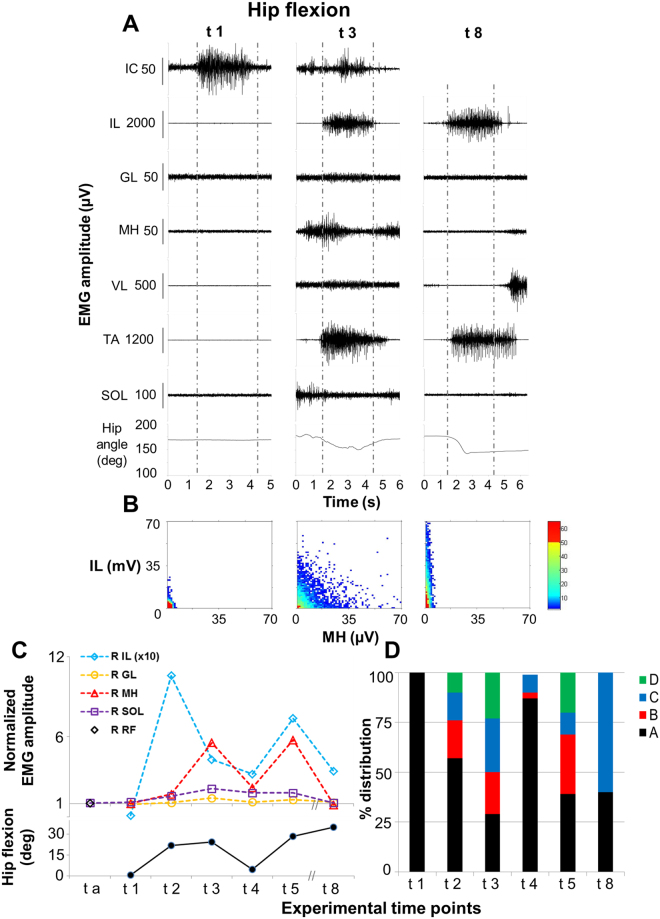
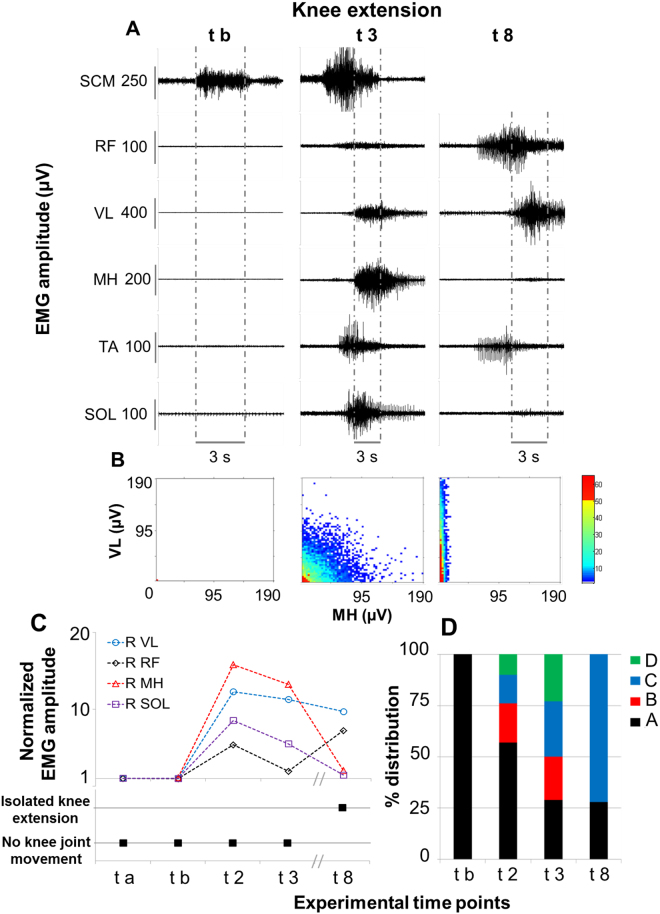
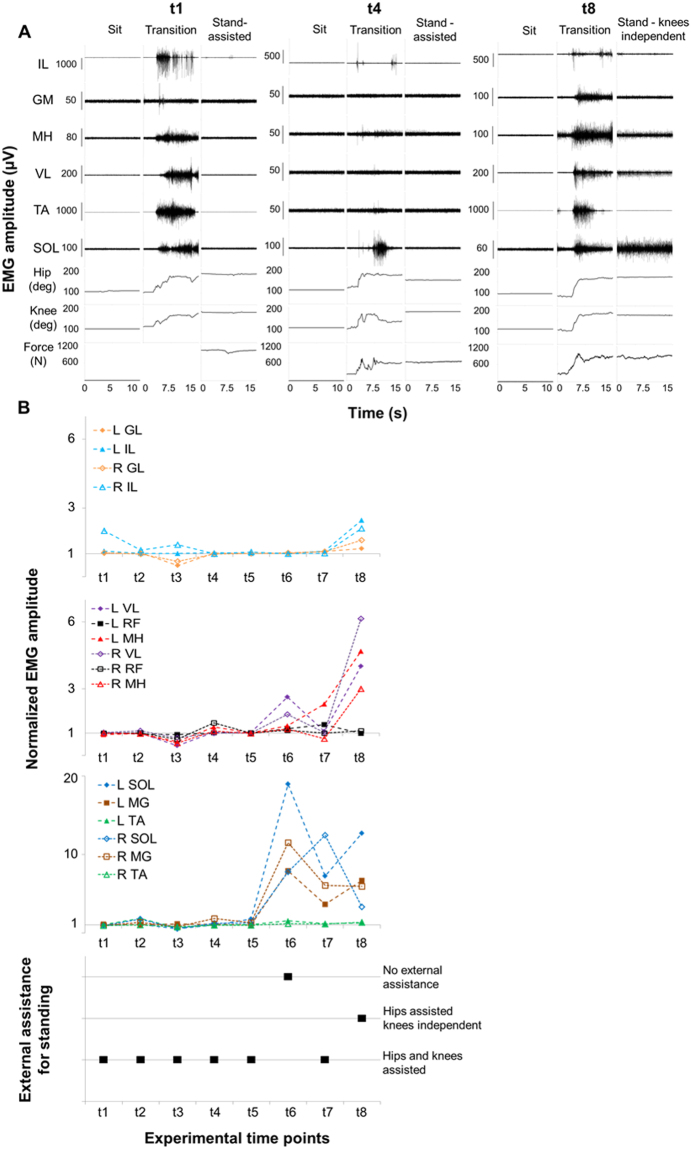
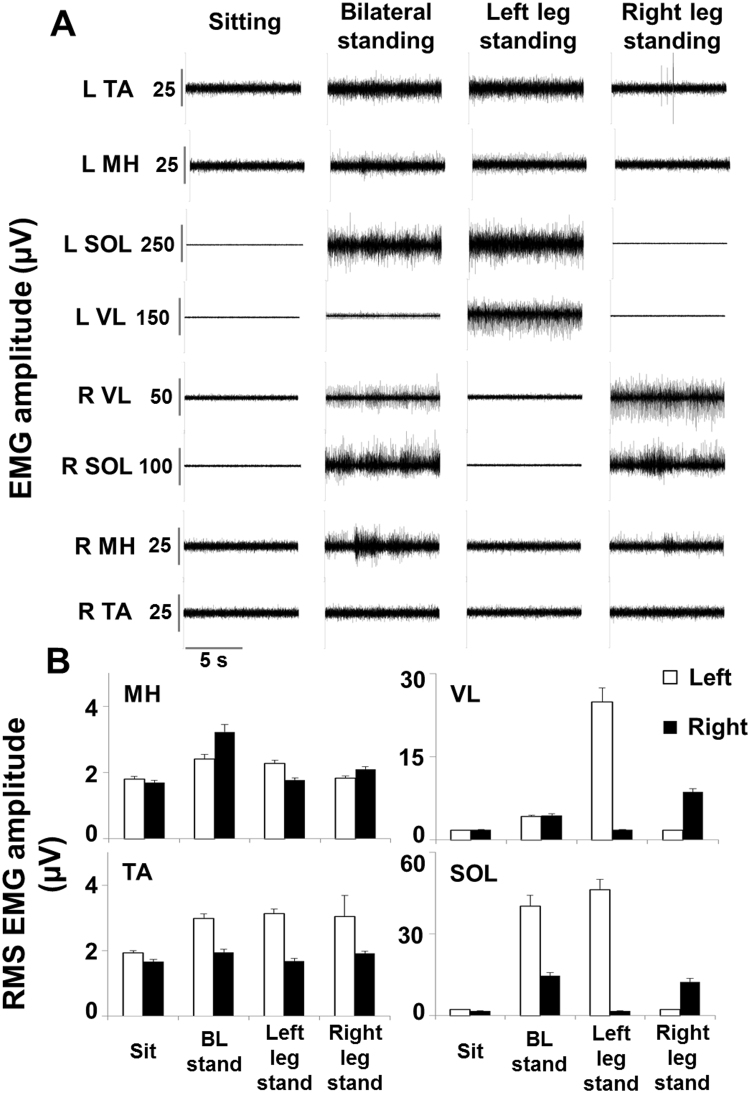
The prognosis for recovery of motor function in motor complete spinal cord injured (SCI) individuals is poor. Our research team has demonstrated that lumbosacral spinal cord epidural stimulation (scES) and activity-based training can progressively promote the recovery of volitional leg movements and standing in individuals with chronic clinically complete SCI. However, scES was required to perform these motor tasks. Herein, we show the progressive recovery of voluntary leg movement and standing without scES in an individual with chronic, motor complete SCI throughout 3.7 years of activity-based interventions utilizing scES configurations customized for the different motor tasks that were specifically trained (standing, stepping, volitional leg movement). In particular, this report details the ongoing neural adaptations that allowed a functional progression from no volitional muscle activation to a refined, task-specific activation pattern and movement generation during volitional attempts without scES. Similarly, we observed the re-emergence of muscle activation patterns sufficient for standing with independent knee and hip extension. These findings highlight the recovery potential of the human nervous system after chronic clinically motor complete SCI.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Waters RL, et al. Recovery following complete paraplegia. Arch. Phys. Med. Rehabil. 1992;73(9):784. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
