

Bacterial Profile and Antibiotic Resistance in Patients with Diabetic Foot Ulcer in Guangzhou, Southern China: Focus on the Differences among Different Wagner's Grades, IDSA/IWGDF Grades, and Ulcer Types
- PMID: 29075293
- PMCID: PMC5623783
- DOI: 10.1155/2017/8694903
Bacterial Profile and Antibiotic Resistance in Patients with Diabetic Foot Ulcer in Guangzhou, Southern China: Focus on the Differences among Different Wagner's Grades, IDSA/IWGDF Grades, and Ulcer Types
Abstract
Objective: To understand the bacterial profile and antibiotic resistance patterns in diabetic foot infection (DFI) in different Wagner's grades, IDSA/IWGDF grades, and different ulcer types in Guangzhou, in order to provide more detailed suggestion to the clinician about the empirical antibiotic choice.
Methods: 207 bacteria were collected from 117 DFIs in Sun Yat-sen Memorial Hospital from Jan.1, 2010, to Dec.31, 2015. The clinical data and microbial information were analyzed.
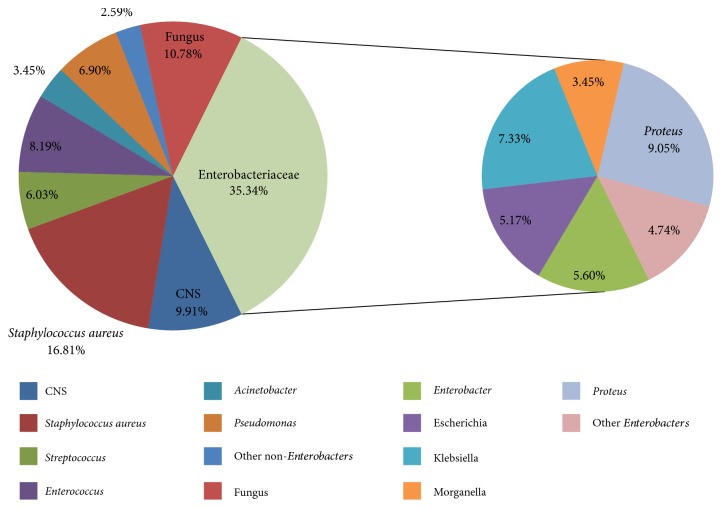
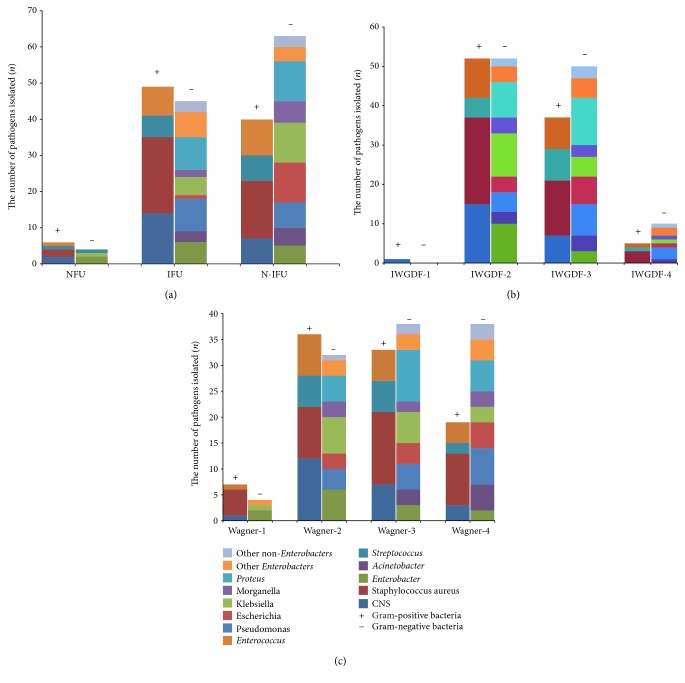
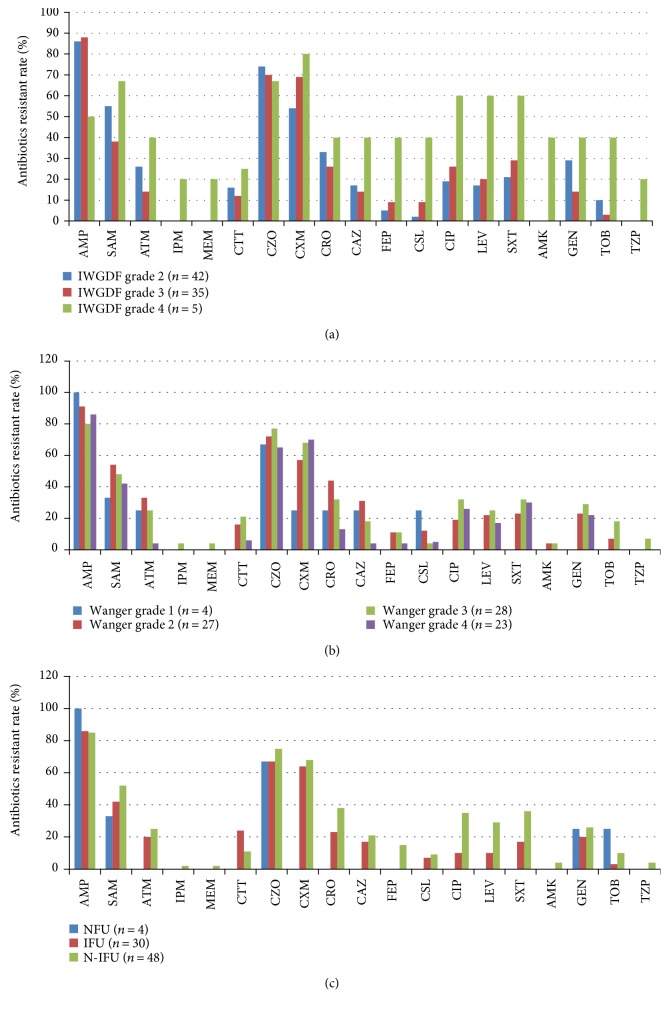
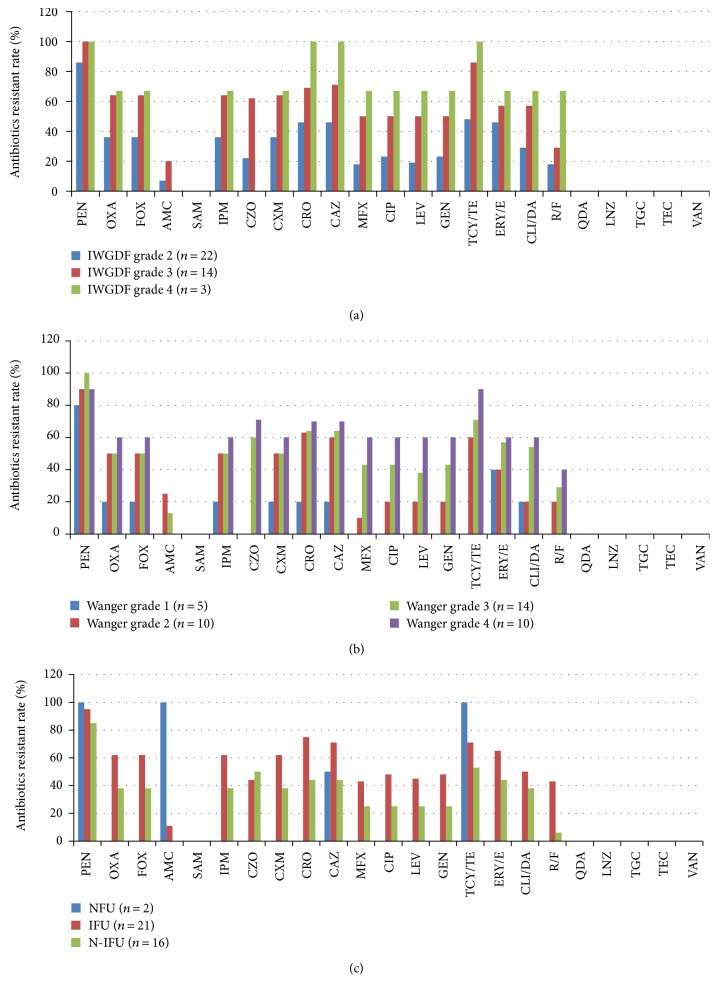
Results: The proportion of Gram-negative bacteria (GNB) was higher than Gram-positive bacteria (GPB) (54.1% versus 45.9%), in which Enterobacteriaceae (73.2%) and Staphylococcus (65.2%) were predominant, respectively. With an increasing of Wagner's grades and IDSA/IWGDF grades, the proportion of GNB bacterial infection, especially Pseudomonas, was increased. Neuro-ischemic ulcer (N-IFU) was more susceptible to GNB infection. Furthermore, with the aggravation of the wound and infection, the antibiotic resistance rates were obviously increased. GPB isolated in ischemic foot ulcer (IFU) showed more resistance than the N-IFU, while GNB isolates were on the opposite.
Conclusions: Different bacterial profiles and antibiotic sensitivity were found in different DFU grades and types. Clinician should try to stay updated in antibiotic resistance pattern of common pathogens in their area. This paper provided them the detailed information in this region.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
