

Characteristics of Donor-Specific Antibodies Associated With Antibody-Mediated Rejection in Lung Transplantation
- PMID: 29075627
- PMCID: PMC5641623
- DOI: 10.3389/fmed.2017.00155
Characteristics of Donor-Specific Antibodies Associated With Antibody-Mediated Rejection in Lung Transplantation
Abstract
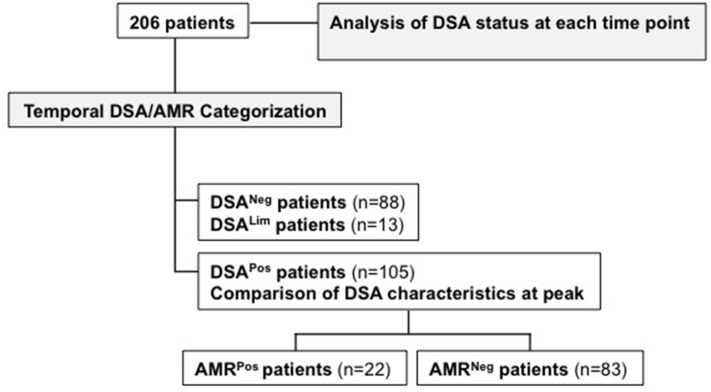
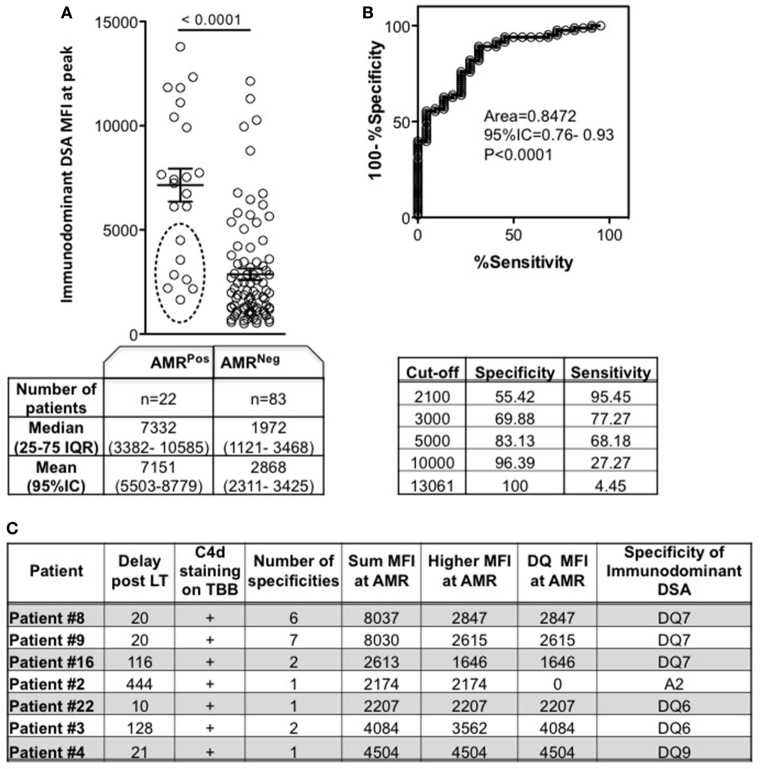
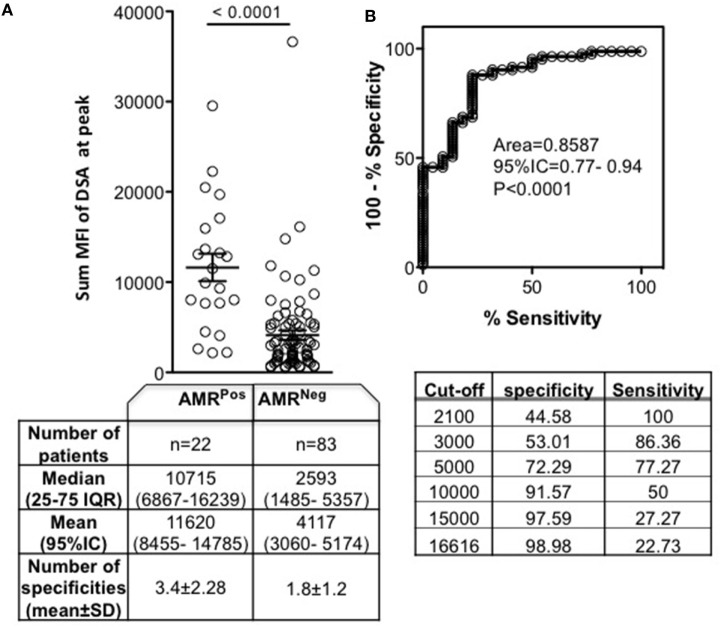
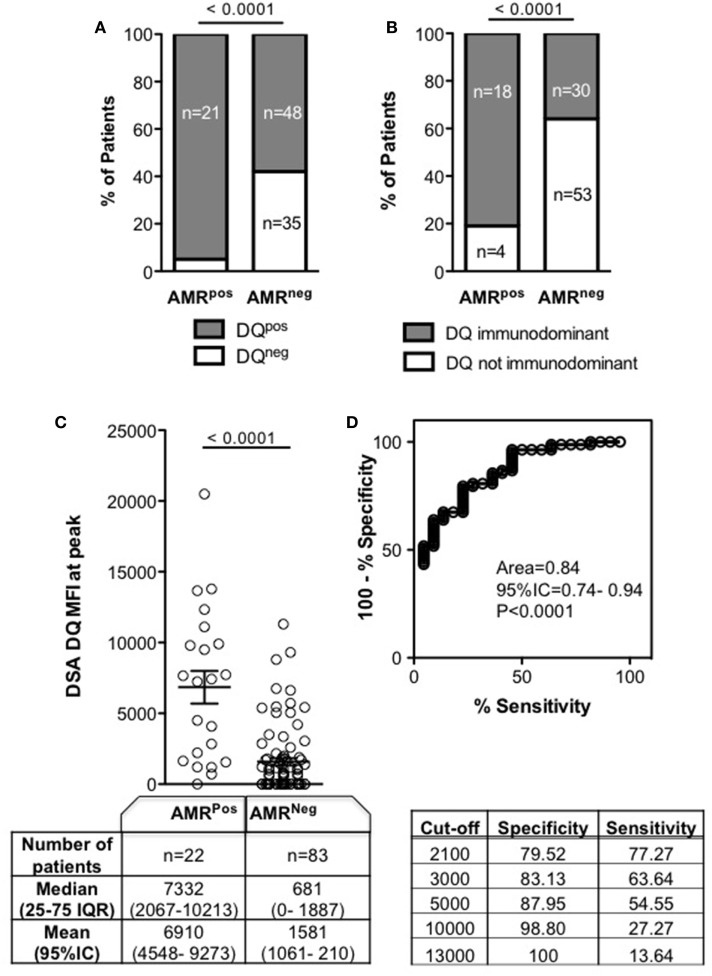
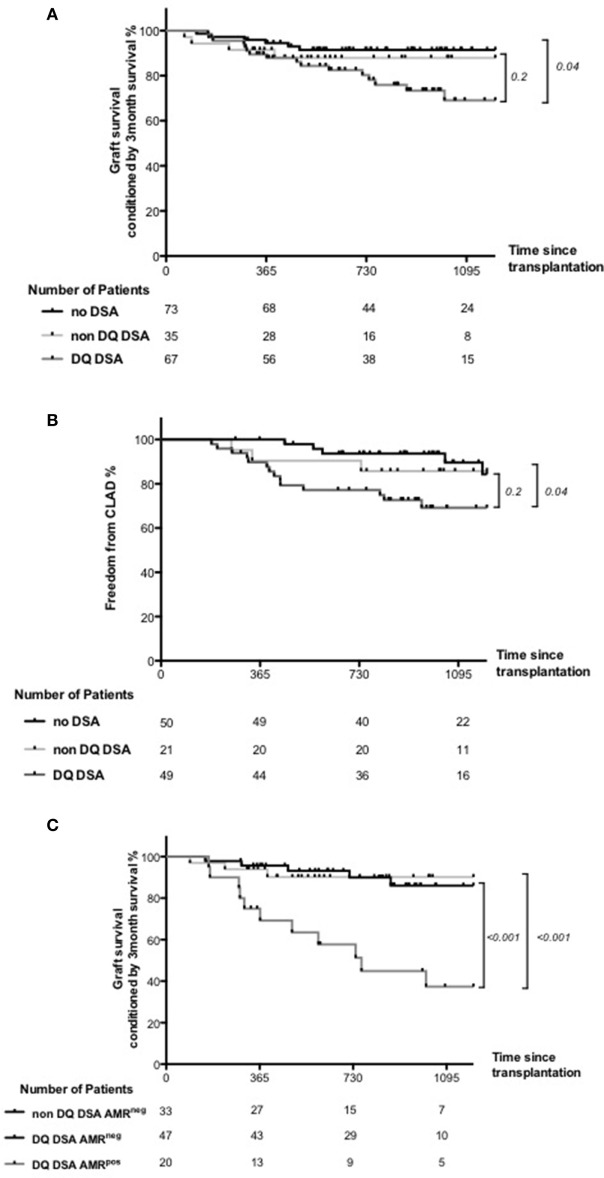
Although donor-specific anti-human leukocyte antigen (HLA) antibodies (DSAs) are frequently found in recipients after lung transplantation (LT), the characteristics of DSA which influence antibody-mediated rejection (AMR) in LT are not fully defined. We retrospectively analyzed 206 consecutive LT patients of our center (2010-2013). DSAs were detected by using luminex single antigen beads assay and mean fluorescence intensity was assessed. Within the study population, 105 patients had positive DSA. Patients with and without AMR (AMRPos, n = 22, and AMRNeg, n = 83, respectively) were compared. AMRPos patients had significantly greater frequencies of anti-HLA DQ DSA (DQ DSA) than AMRNeg patients (95 vs 58%, respectively, p < 0.0001). Compared to AMRNeg patients, AMRPos patients had higher DQ DSA sum MFI [7,332 (2,067-10,213) vs 681 (0-1,887), p < 0.0001]. DQ DSA when associated with AMR, had more frequent graft loss and chronic lung allograft dysfunction (CLAD). These data suggest (i) that DSA characteristics clearly differ between AMRPos and AMRNeg patients and (ii) the deleterious impact of DQ DSA on clinical outcome.
Keywords: HLA; antibody mediated rejection; clinical outcome; donor-specific antibodies; lung transplant.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials