

MELD score and AST-to-platelet ratio index (APRI) predict long-term survival in patients with a small hepatocellular carcinoma following non-transplant therapies: a pilot study
- PMID: 29075672
- PMCID: PMC5654577
- DOI: 10.20517/2394-5079.2017.06
MELD score and AST-to-platelet ratio index (APRI) predict long-term survival in patients with a small hepatocellular carcinoma following non-transplant therapies: a pilot study
Abstract
Aim: Liver transplantation (LT) is the most effective treatment for long-term survival from hepatocellular carcinoma (HCC); however, insufficient donors limit therapy. We sought to identify characteristics that predicted long-term survival after non-transplant therapies in patients with small HCC.
Methods: In a database of 1,050 HCC patients, we identified those with single HCC ≤ 3.0 cm, who underwent hepatic resection (HR, n = 16), radiofrequency ablation (RFA, n = 55), or LT (n = 23) with 5-years follow-up. Survival and odds-ratios for survival (OS) after HR/RFA were calculated for MELD score, platelet count, creatinine, albumin, AST/Platelet Ratio Index (APRI), INR, and bilirubin.
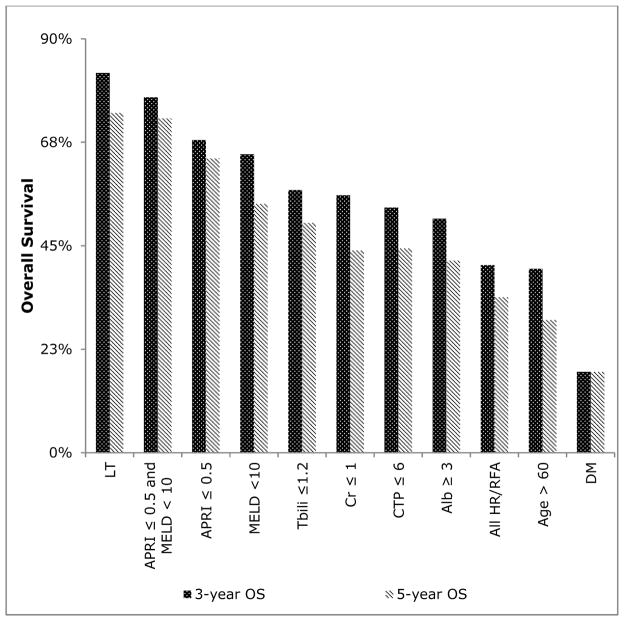
Results: LT patients had 3 and 5-year OS of 82.6% and 73.9% compared to HR/RFA patients with 3 and 5-year OS of 40.8% and 33.8%. The strongest predictors of survival after HR/RFA were MELD < 10 (OR 4.43, 95% CI 1.85-10.58) and APRI ≤ 0.5 (OR 4.25, 95% CI 1.63-11.08). HR/RFA patients with both MELD < 10 and APRI ≤ 0.5 had 3- and 5-year OS of 77.3% and 72.7%.
Conclusion: Patients with MELD < 10 and APRI ≤ 0.5 who undergo HR/RFA have survival approaching LT. Perhaps patients who meet these criteria can safely undergo non-transplant therapy and donor livers can be allocated to patients with a greater need.
Keywords: Hepatocellular carcinoma; ablation; liver resection; transplant.
Figures
Similar articles
-
Preoperative albumin-bilirubin grade combined with aspartate aminotransferase-to-platelet count ratio index predict outcomes of patients with hepatocellular carcinoma within Milan criteria after liver resection.Biosci Trends. 2019 May 12;13(2):176-181. doi: 10.5582/bst.2019.01088. Epub 2019 Apr 27. Biosci Trends. 2019. PMID: 31061272
-
Estimation of hepatocellular carcinoma mortality using aspartate aminotransferase to platelet ratio index.J Gastrointest Oncol. 2020 Apr;11(2):291-297. doi: 10.21037/jgo.2018.11.01. J Gastrointest Oncol. 2020. PMID: 32399270 Free PMC article.
-
Long-term outcomes of ablation, liver resection, and liver transplant as first-line treatment for solitary HCC of 3 cm or less using an intention-to-treat analysis: A retrospective cohort study.Ann Med Surg (Lond). 2022 Apr 20;77:103645. doi: 10.1016/j.amsu.2022.103645. eCollection 2022 May. Ann Med Surg (Lond). 2022. PMID: 35637985 Free PMC article.
-
Appropriate treatment modality for solitary small hepatocellular carcinoma: Radiofrequency ablation vs. resection vs. transplantation?Clin Mol Hepatol. 2019 Dec;25(4):354-359. doi: 10.3350/cmh.2018.0096. Epub 2019 Apr 22. Clin Mol Hepatol. 2019. PMID: 31006225 Free PMC article. Review.
-
Predictors of intermediate-term survival with destination locoregional therapy of hepatocellular cancer in patients either ineligible or unwilling for liver transplantation.J Gastrointest Oncol. 2017 Oct;8(5):885-889. doi: 10.21037/jgo.2017.07.05. J Gastrointest Oncol. 2017. PMID: 29184693 Free PMC article. Review.
Cited by
-
Overexpression of miRNA-21 Promotes the Proliferation and Invasion in Hepatocellular Carcinoma Cells via Suppressing SMAD7.Technol Cancer Res Treat. 2019 Jan 1;18:1533033819878686. doi: 10.1177/1533033819878686. Technol Cancer Res Treat. 2019. Retraction in: Technol Cancer Res Treat. 2025 Jan-Dec;24:15330338251363346. doi: 10.1177/15330338251363346. PMID: 31554487 Free PMC article. Retracted.
-
Prognostic value of aspartate aminotransferase to platelet ratio index as a noninvasive biomarker in patients with hepatocellular carcinoma: a meta-analysis.Cancer Manag Res. 2018 Aug 29;10:3023-3032. doi: 10.2147/CMAR.S174095. eCollection 2018. Cancer Manag Res. 2018. PMID: 30214297 Free PMC article.
-
Radiofrequency ablation for peribiliary hepatocellular carcinoma: propensity score matching analysis.Insights Imaging. 2025 Feb 19;16(1):45. doi: 10.1186/s13244-025-01919-5. Insights Imaging. 2025. PMID: 39971810 Free PMC article.
-
Individualized Ablation of Hepatocellular Carcinoma: Tailored Approaches across the Phenotype Spectrum.Semin Intervent Radiol. 2019 Oct;36(4):287-297. doi: 10.1055/s-0039-1698755. Epub 2019 Oct 31. Semin Intervent Radiol. 2019. PMID: 31680719 Free PMC article. Review.
-
Assessment of Prognostic Value of Aspartate Aminotransferase-to-Platelet Ratio Index in Patients With Hepatocellular Carcinoma: Meta-Analysis of 28 Cohort Studies.Front Med (Lausanne). 2021 Nov 26;8:756210. doi: 10.3389/fmed.2021.756210. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34901068 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J of Cancer. 2015;136:E359–86. - PubMed
-
- Belghiti J. Transplantation for liver tumors. Semin Oncol. 2005;32:29–32. - PubMed
-
- Yao FY, Bass NM, Nikolai B, Davern TJ, Kerlan R, Wu V, Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: analysis of survival according to the intention-to-treat principle and dropout from the waiting list. Liver Transpl. 2002;8:873–83. - PubMed
-
- Adam R, Bhangui P, Vibert E, Azoulay D, Pelletier G, Duclos-Vallée JC, Samuel D, Guettier C, Castaing D. Resection or transplantation for early hepatocellular carcinoma in a cirrhotic liver: does size define the best oncological strategy? Ann Surg. 2012;256:883–91. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources