

Multidisciplinary Clinic Management of Head and Neck Cancer
- PMID: 29075744
- PMCID: PMC5824300
- DOI: 10.1001/jamaoto.2017.1855
Multidisciplinary Clinic Management of Head and Neck Cancer
Abstract
Importance: Contemporary management of head and neck cancer involves professionals from multiple specializations. Streamlined care that reduces delays yet allows for comprehensive evaluation is needed.
Objective: To evaluate a single-day, single-appointment, multidisciplinary head and neck clinic model for reduction in treatment delay and comprehensiveness of care.
Design, Setting, and Participants: A retrospective cohort analysis was conducted from June 1, 2015, to July 31, 2016, of outpatients at a single, academic medical center.
All eligible outpatients seen in either the multiple-appointment, traditional clinic (n = 73) or the single-day multidisciplinary clinic (MDC) (n = 68) were included. Patients with new squamous cell carcinoma of the oropharynx, hypopharynx, sinonasal tract, and larynx, along with any mucosal site recurrence were eligible for the study.
Main Outcomes and Measures: Primary outcomes were delays between tertiary clinic referral or first appointment and treatment initiation in the MDC compared with the traditional clinic. Secondary outcomes were complete evaluations prior to treatment, enrollment in trials and registries, and rate of patient leak, defined as initiating therapy and then transferring to another center before completion. Outcome selection and hypothesis generation were performed a priori.
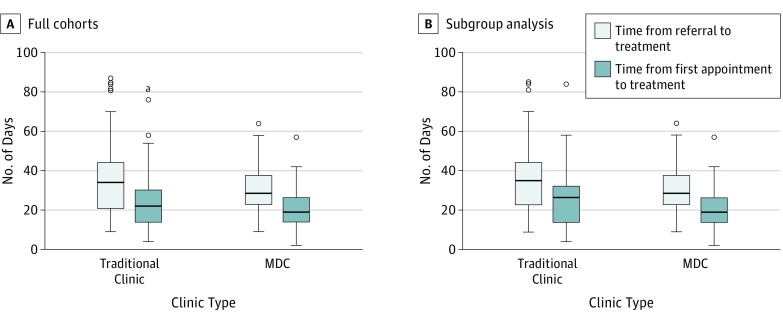
Results: Patient factors and tumor characteristics were similar between the traditional clinic cohort (19 women and 54 men; mean [SD] age, 64.0 [10.2] years) and the MDC cohort (8 women and 60 men; mean [SD] age, 61.0 [8.9] years). The MDC cohort had significantly fewer instances of delay greater than 30 days from referral to treatment initiation (28 [41%] vs 43 [59%]) and first appointment to treatment initiation (7 [10%] vs 17 [23%]). Actual median days in these categories were significantly different between the 2 clinic types after the patients in the traditional clinic who saw only a surgeon before treatment initiation were excluded (MDC, 28 days vs traditional, 35 days; median difference, –5 days; 95% CI, –11 to –1).
Conclusions and Relevance: Coordination of the management of head and neck cancer is complex. Treatment is time sensitive, and frequently clinician resources are limited. This MDC model was associated with improved efficiency and completeness of care.
Conflict of interest statement
Figures

Comment in
-
Multidisciplinary Clinical Treatment of Head and Neck Cancer-Reply.JAMA Otolaryngol Head Neck Surg. 2018 May 1;144(5):461. doi: 10.1001/jamaoto.2017.3451. JAMA Otolaryngol Head Neck Surg. 2018. PMID: 29543957 No abstract available.
-
Multidisciplinary Clinical Treatment of Head and Neck Cancer.JAMA Otolaryngol Head Neck Surg. 2018 May 1;144(5):460-461. doi: 10.1001/jamaoto.2017.3437. JAMA Otolaryngol Head Neck Surg. 2018. PMID: 29543958 No abstract available.
References
-
- Hong NJ, Wright FC, Gagliardi AR, Paszat LF. Examining the potential relationship between multidisciplinary cancer care and patient survival: an international literature review. J Surg Oncol. 2010;102(2):125-134. - PubMed
-
- Taylor C, Munro AJ, Glynne-Jones R, et al. Multidisciplinary team working in cancer: what is the evidence? BMJ. 2010;340:c951. - PubMed
-
- National Comprehensive Cancer Network NCCN guidelines for head and neck cancer care. https://www.nccn.org/store/login/login.aspx?ReturnURL=http://www.nccn.or.... Accessed July 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
