

Efficacy of depatuxizumab mafodotin (ABT-414) monotherapy in patients with EGFR-amplified, recurrent glioblastoma: results from a multi-center, international study
- PMID: 29075855
- PMCID: PMC5686264
- DOI: 10.1007/s00280-017-3451-1
Efficacy of depatuxizumab mafodotin (ABT-414) monotherapy in patients with EGFR-amplified, recurrent glioblastoma: results from a multi-center, international study
Abstract
Purpose: Patients with recurrent glioblastoma (rGBM) have a poor prognosis. Epidermal growth factor receptor (EGFR) gene amplification is present in ~ 50% of glioblastomas (GBMs). Depatuxizumab mafodotin (depatux-m), formerly ABT-414, is an antibody-drug conjugate that preferentially binds cells with EGFR amplification, is internalized and releases a potent antimicrotubule agent, monomethyl auristatin F (MMAF). Here we report the safety, pharmacokinetics, and efficacy of depatux-m monotherapy at the recommended Phase 2 dose (RPTD) in patients with EGFR-amplified, rGBM.
Methods: M12-356 (NCT01800695) is an open-label study with three escalation and expansion cohorts. Sixty-six patients with EGFR-amplified, rGBM were treated with depatux-m monotherapy at 1.25 mg/kg intravenously every 2 weeks. Adults with measurable rGBM, who were bevacizumab-naïve, with EGFR amplification were eligible.
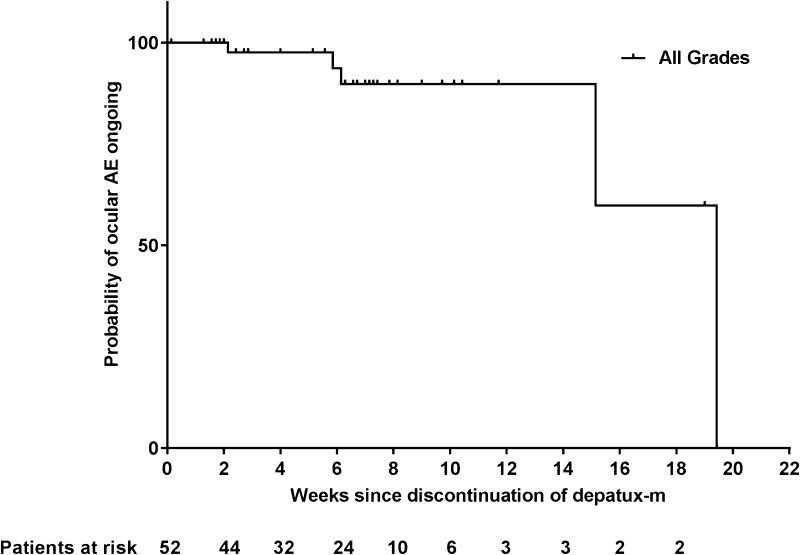
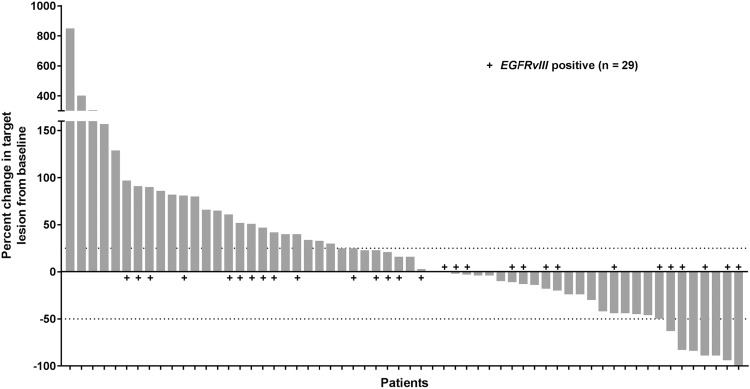
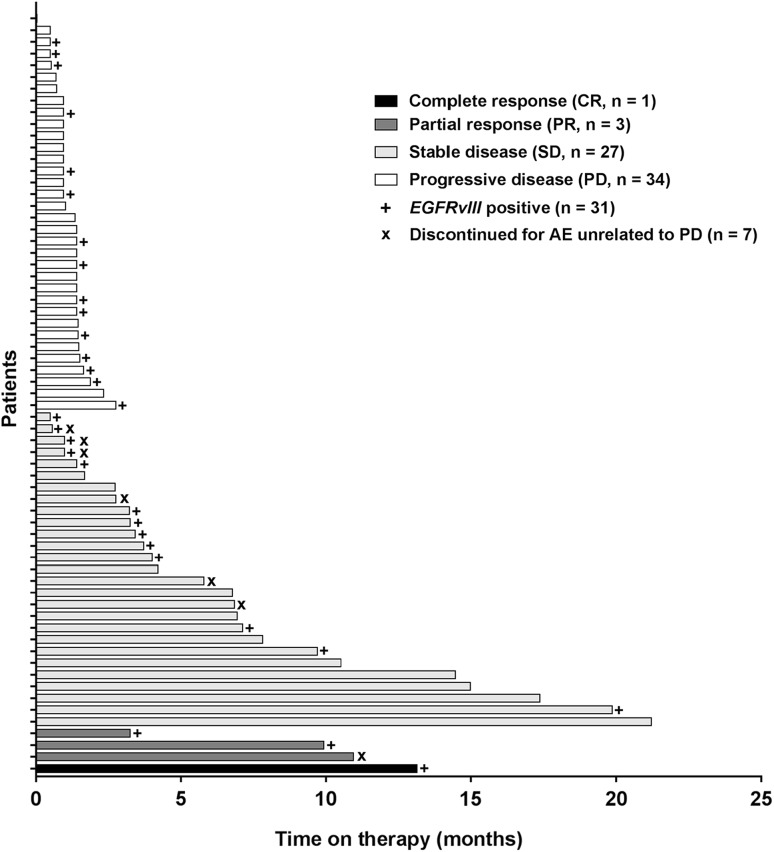
Results: Among 66 patients, median age was 58 years (range 35-80). All patients were previously treated with radiotherapy/temozolomide. The most common adverse events (AEs) were eye related (91%), including blurred vision (65%), dry eye (29%), keratitis, and photophobia (27% each). Grade 3/4 AEs occurred in 42% of all patients, and ocular Grade 3/4 AEs occurred in 33% of patients overall. One patient (2%) had a Grade 4 ocular AE. Ocular AEs were manageable and usually resolved once treatment with depatux-m ceased. The objective response rate was 6.8%, the 6-month progression-free survival rate was 28.8%, and the 6-month overall survival rate was 72.5%.
Conclusion: Depatux-m monotherapy displayed frequent but mostly Grade 1/2 ocular toxicities. A PFS6 of 28.8% was observed in this rGBM population, warranting further study.
Keywords: ABT-414; Antibody–drug conjugate; Depatuxizumab mafodotin; EGFR; Recurrent glioblastoma.
Conflict of interest statement
Funding
AbbVie provided financial support for this study (NCT01800695) and participated in the design, study conduct, analysis and interpretation of the data, as well as the writing, review, and approval of the manuscript. All authors were involved in the data gathering, analysis, review, interpretation and manuscript preparation and approval.
Conflict of interest
Martin van den Bent: received honoraria from Roche, AbbVie, Celldex, Merck Ag, Cavion, Actelion, BMS, Blue Earth Diagnostics and Novartis; received research funding from AbbVie. Hui K. Gan: has an investigator-initiated study with AbbVie; received travel support and research funding from AbbVie; received honoraria from Pfizer, BMS, and Merck Serono; affiliated with the Ludwig Institute for Cancer Research. Andrew B. Lassman: in the last 12 months received personal compensation from WebMD, Sapience Therapeutics, Genentech, Italian Association for Cancer Research, AbbVie, AstraZeneca, Novocure, and Kadmon; additional travel support from Karyopharm, AstraZeneca, Abbvie, Bioclinica, Genentech, and VBI Vaccines; and research support from RTOG Foundation, Genentech, Amgen, AbbVie, Novartis, Karyopharm, Celldex, NW Biotherapeutics, Plexxicon, Pfizer, Agenus, Medimmune, Boehringer Ingelheim, Angiochem, Novocure, Stemline, E-Therapeutics, Millennium. Priya Kumthekar: Consultant for AbbVie. Ryan Merrell: Serves on a Scientific Advisory Board for AbbVie. Nicholas Butowski: Received honoraria from and has a consulting or advisory role with, Roche/Genentech, Medicenna, VBL Theraputics, Omniox; is involved in speakers’ bureaus with Roche and Merck; received research funding from Insys. Zarnie Lwin: Has served on Abbvie Scientific Advisory Board and received honoraria. Tom Mikkelsen: No potential conflicts of interest to disclose. Louis B. Nabors: Serves on a Scientific Advisory Board for Cavion, Merck, and BMS; investigator for AbbVie. Kyriakos P. Papadopoulos: Received research funding from AbbVie, MedImmune, Daiichi Sankyo, GlaxoSmithKline, Onyx, Sanofi, Novartis. Marta Penas-Prado: No potential conflicts of interest to disclose. John Simes: Received research funding for an investigator-initiated trial from AbbVie. Helen Wheeler: Investigator for AbbVie. Tobias Walbert: Serves on a Scientific Advisory Board for Novocure. Andrew M. Scott: Received research funding and travel support from AbbVie; received research funding from Daiichi-Sankyo; is a consultant and has stock in Life Science Pharmaceuticals; is affiliated with the Ludwig Institute for Cancer Research. Erica Gomez, Ho-Jin Lee, Lisa Roberts-Rapp, Hao Xiong, Earle Bain, Peter J. Ansell, Kyle D. Holen, David Maag: Employees of AbbVie and may own stock. David A. Reardon: Received honoraria from and has a consulting or advisory role with Abbvie, Bristol Myers Squibb, Cavion, Celldex, Inovio, Merck, Novartis, Roche/Genentech, Amgen, Novocure, Oxigene, Regeneron and Stemline Therapeutics; is involved in speakers’ bureaus with Roche and Merck; received research funding from Incyte, Midatech and Celldex.
Ethical approval
This article does not contain any study with animals performed by any of the authors.
Human rights and animal statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, Mokhtari K, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M, Lacombe D, Cairncross JG, Mirimanoff RO, European Organisation for R, Treatment of Cancer Brain T, Radiation Oncology G, National Cancer Institute of Canad. a Clinical Trials G Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. doi: 10.1016/S1470-2045(09)70025-7. - DOI - PubMed
-
- Ostrom QT, Gittleman H, Liao P, Rouse C, Chen Y, Dowling J, Wolinsky Y, Kruchko C, Barnholtz-Sloan J. CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. Neuro Oncol. 2014;16(Suppl 4):iv1-63. doi: 10.1093/neuonc/nou223. - DOI - PMC - PubMed
-
- Lamborn KR, Yung WK, Chang SM, Wen PY, Cloughesy TF, DeAngelis LM, Robins HI, Lieberman FS, Fine HA, Fink KL, Junck L, Abrey L, Gilbert MR, Mehta M, Kuhn JG, Aldape KD, Hibberts J, Peterson PM, Prados MD, North American Brain Tumor C Progression-free survival: an important end point in evaluating therapy for recurrent high-grade gliomas. Neuro Oncol. 2008;10(2):162–170. doi: 10.1215/15228517-2007-062. - DOI - PMC - PubMed
-
- Brennan CW, Verhaak RG, McKenna A, Campos B, Noushmehr H, Salama SR, Zheng S, Chakravarty D, Sanborn JZ, Berman SH, Beroukhim R, Bernard B, Wu CJ, Genovese G, Shmulevich I, Barnholtz-Sloan J, Zou L, Vegesna R, Shukla SA, Ciriello G, Yung WK, Zhang W, Sougnez C, Mikkelsen T, Aldape K, Bigner DD, Van Meir EG, Prados M, Sloan A, Black KL, Eschbacher J, Finocchiaro G, Friedman W, Andrews DW, Guha A, Iacocca M, O’Neill BP, Foltz G, Myers J, Weisenberger DJ, Penny R, Kucherlapati R, Perou CM, Hayes DN, Gibbs R, Marra M, Mills GB, Lander E, Spellman P, Wilson R, Sander C, Weinstein J, Meyerson M, Gabriel S, Laird PW, Haussler D, Getz G, Chin L, Network TR. The somatic genomic landscape of glioblastoma. Cell. 2013;155(2):462–477. doi: 10.1016/j.cell.2013.09.034. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
