

Seroma following transabdominal preperitoneal patch plasty (TAPP): incidence, risk factors, and preventive measures
- PMID: 29075973
- PMCID: PMC5897456
- DOI: 10.1007/s00464-017-5912-3
Seroma following transabdominal preperitoneal patch plasty (TAPP): incidence, risk factors, and preventive measures
Abstract
Background: The reported range of seroma formation in the literature after TEP repair is between 0.5 and 12.2% and for TAPP between 3.0 and 8.0%. Significant clinical factors associated with seroma formation include old age, a large hernia defect, an extension of the hernia sac into the scrotum, as well as the presence of a residual indirect sac. Seroma formation is a frequent complication of laparoendoscopic mesh repair of moderate to large-size direct (medial) inguinal hernia defects. This present analysis of data from the Herniamed Hernia Registry now explores the influencing factors for seroma formation in male patients after TAPP repair of primary unilateral inguinal hernia.
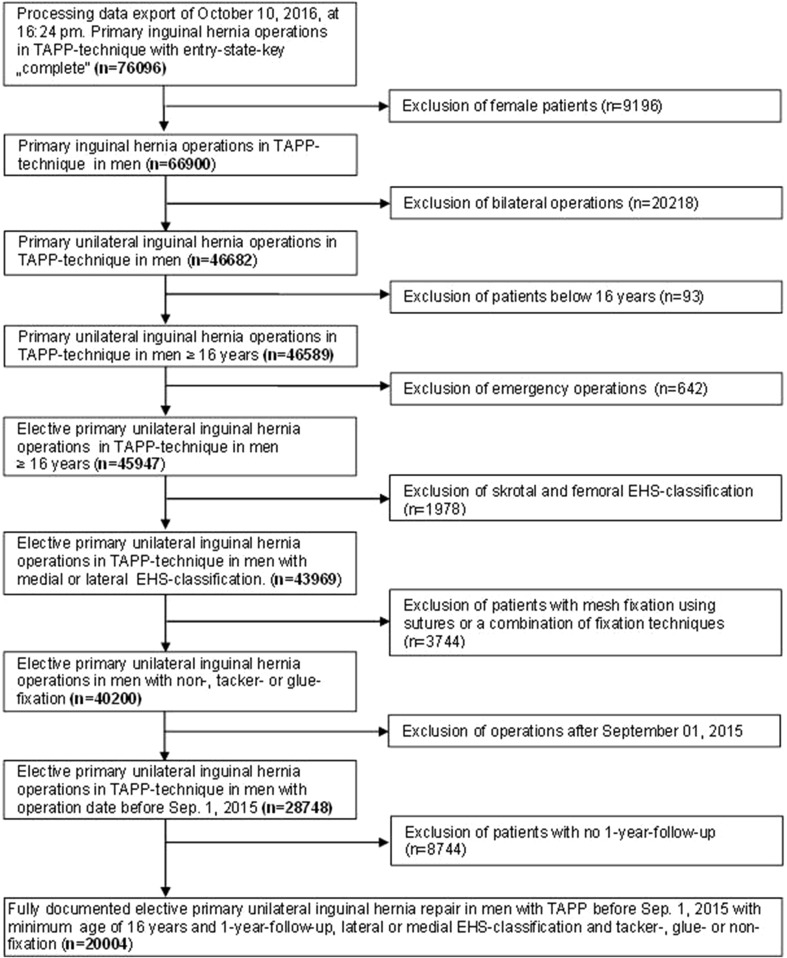
Methods: In total, 20,004 male patients with TAPP repair of primary unilateral inguinal hernia were included in uni- and multivariable analysis.
Results: Univariable analysis revealed the highly significant impact of the fixation technique on the seroma rate (non-fixation 0.7% vs. tacks 2.1% vs. glue 3.9%; p < 0.001). Multivariable analysis showed that glue compared to tacks (OR 2.077 [1.650; 2.613]; p < 0.001) and non-fixation (OR 5.448 [4.056; 7.317]; p < 0.001) led to an increased seroma rate. A large hernia defect (III vs. I: OR 2.868 [1.815; 4.531]; p < 0.001; II vs. I: OR 2.157 [1.410; 3.300]; p < 0.001) presented a significantly higher risk of seroma formation. Likewise, medial compared to lateral inguinal hernias had a higher seroma rate (OR 1.272 [1.020; 1.585]; p = 0.032).
Conclusions: Mesh fixation with tacks or glue, a larger hernia defect, and medial defect localization present a higher risk for seroma development in TAPP inguinal hernia repair.
Keywords: Complications; Inguinal hernia; Mesh fixation; Seroma; TAPP.
Conflict of interest statement
R. Bittner, D. Adolf, R. Fortelny, H. Niebuhr, F. Mayer, C. Schug-Pass have no conflicts of interest or financial ties to disclose.
References
-
- Bittner R, Arregui ME, Bisgaard T, Dudai M, Ferzli GS, Fitzgibbons RL, Fortelny RH, Klinge U, Köckerling F, Kuhry E, Kukleta J, Lomanto D, Misra MC, Montgomery A, Morales-Conde S, Reinpold W, Rosenberg J, Sauerland S, Schug-Pass C, Singh K, Timoney M, Weyhe D, Chowbey P. Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia [International Endohernia Society (IEHS)] Surg Endosc. 2011;25(9):2773–2843. doi: 10.1007/s00464-011-1799-6. - DOI - PMC - PubMed
-
- Bittner R, Montgomery MA, Arregui E, Bansal V, Bingener J, Bisgaard T, Buhck H, Dudai M, Ferzli GS, Fitzgibbons RJ, Frotelny RH, Grimes KL, Klinge U, Köckerling F, Kumar S, Kukleta J, Lomanto D, Misra MC, Morales-Conde S, Reinpold W, Rosenberg J, Signh K, Timoney M, Weyhe D, Chowbey P. International Endohernia Society update of guidelines on laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia (International Endohernia Society) Surg Endosc. 2015;29(2):289–321. doi: 10.1007/s00464-014-3917-8. - DOI - PMC - PubMed
-
- Poelman MM, van den Heuvel B, Deelder JD, Abis GS, Beudeker N, Bittner R, Campanelli G, van Dam D, Dwars BJ, Eker HH, Fingerhut A, Khatkov I, Köckerling F, Kukleta JF, Miserez M, Montgomery A, Munoz Brands RM, Morales-Conde S, Muysoms FE, Soltes M, Tromp W, Yavuz Y, Bonjer HJ. EAES consensus development conference on endoscopic repair of groin. Hernias Surg Endosc. 2013;27(10):3505–3519. doi: 10.1007/s00464-013-3001-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
