

Non-Immune Hydrops Fetalis: Do Placentomegaly and Polyhydramnios Matter?
- PMID: 29076544
- PMCID: PMC6029704
- DOI: 10.1002/jum.14462
Non-Immune Hydrops Fetalis: Do Placentomegaly and Polyhydramnios Matter?
Abstract
Objectives: Polyhydramnios and placentomegaly are commonly observed in nonimmune hydrops fetalis (NIHF); however, whether their ultrasonographic identification is relevant for prognosis is controversial. We evaluated outcomes of fetal or neonatal death and preterm birth (PTB) in cases of NIHF alone and in those with polyhydramnios and/or placentomegaly (P/PM).
Methods: We conducted a retrospective cohort of singletons with NIHF evaluated between 1994 and 2013. Nonimmune hydrops fetalis was defined as 2 or more abnormal fluid collections, including ascites, pericardial effusion, pleural effusion, and skin edema. Primary outcomes were intrauterine fetal demise (IUFD) and neonatal death. Secondary outcomes were PTB (<37, < 34, and <28 weeks) and spontaneous PTB. Outcomes were compared between cases of NIHF alone and NIHF with P/PM.
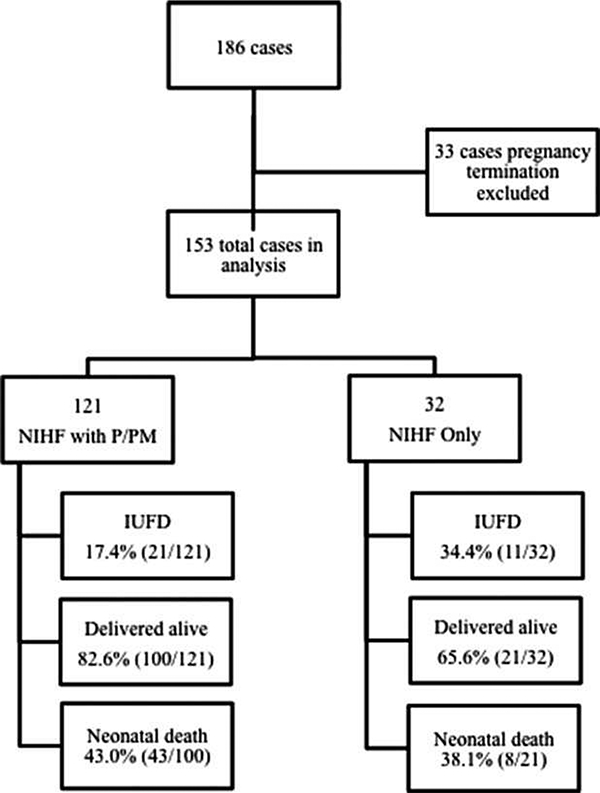
Results: A total of 153 cases were included; 21% (32 of 153) had NIHF alone, and 79% (121 of 153) had NIHF with P/PM. There was no significant difference in neonatal death (38.1% versus 43.0%; P = .809) between the groups. Intrauterine fetal demise was seen more frequently in NIHF alone (34.4% versus 17.4%; P = .049). Nonimmune hydrops fetalis-with-P/PM cases were more likely to deliver before 37 weeks (80.0% versus 57.1%; P = .045) and before 34 weeks (60.0% versus 28.6%; P = .015) and to have spontaneous PTB (64.4% versus 33.3%; P = .042). Adjusted odds ratios accounting for the etiology of NIHF supported these findings, with the exception of IUFD.
Conclusions: Compared to NIHF alone, pregnancies with NIHF and P/PM had a lower risk of IUFD and were at increased risk of PTB (<37 and <34 weeks) and spontaneous PTB. This information may help providers in counseling patients with NIHF and supports the need for close antenatal surveillance.
Keywords: intrauterine demise; neonatal death; nonimmune hydrops fetalis; obstetrics; placentomegaly; polyhydramnios; preterm birth.
© 2017 by the American Institute of Ultrasound in Medicine.
Figures
References
-
- Society for Maternal-Fetal Medicine; Norton ME, Chauhan SP, Dashe JS. Society for Maternal-Fetal Medicine (SMFM) clinical guideline #7: nonimmune hydrops fetalis. Am J Obstet Gynecol 2015; 212:127–139. - PubMed
-
- Bellini C, Donarini G, Paladini D, et al. Etiology of non-immune hydrops fetalis: an update. Am J Med Genet A 2015; 167A:1082–1088. - PubMed
-
- Santo S, Mansour S, Thilaganathan B, et al. Prenatal diagnosis of nonimmune hydrops fetalis: what do we tell the parents? Prenat Diagn 2011;31:186–195. - PubMed
-
- Nakayama H, Kukita J, Hikino S, Nakano H, Hara T. Long-term outcome of 51 liveborn neonates with non-immune hydrops fetalis. Acta Paediatr 1999; 88:24–28. - PubMed
-
- Moreno CA, Kanazawa T, Barini R, et al. Non-immune hydrops fetalis: a prospective study of 53 cases. Am J Med Genet A 2013; 161A: 3078–3086. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
