

Systematic review of community-based, school-based, and combined delivery modes for reaching school-aged children in mass drug administration programs for schistosomiasis
- PMID: 29077723
- PMCID: PMC5678727
- DOI: 10.1371/journal.pntd.0006043
Systematic review of community-based, school-based, and combined delivery modes for reaching school-aged children in mass drug administration programs for schistosomiasis
Abstract
Background: The mainstay of current schistosomiasis control programs is mass preventive chemotherapy of school-aged children with praziquantel. This treatment is delivered through school-based, community-based, or combined school- and community-based systems. Attaining very high coverage rates for children is essential in mass schistosomiasis treatment programs, as is ensuring that there are no persistently untreated subpopulations, a potential challenge for school-based programs in areas with low school enrollment. This review sought to compare the different treatment delivery methods based both on their coverage of school-aged children overall and on their coverage specifically of non-enrolled children. In addition, qualitative community or programmatic factors associated with high or low coverage rates were identified, with suggestions for overall coverage improvement.
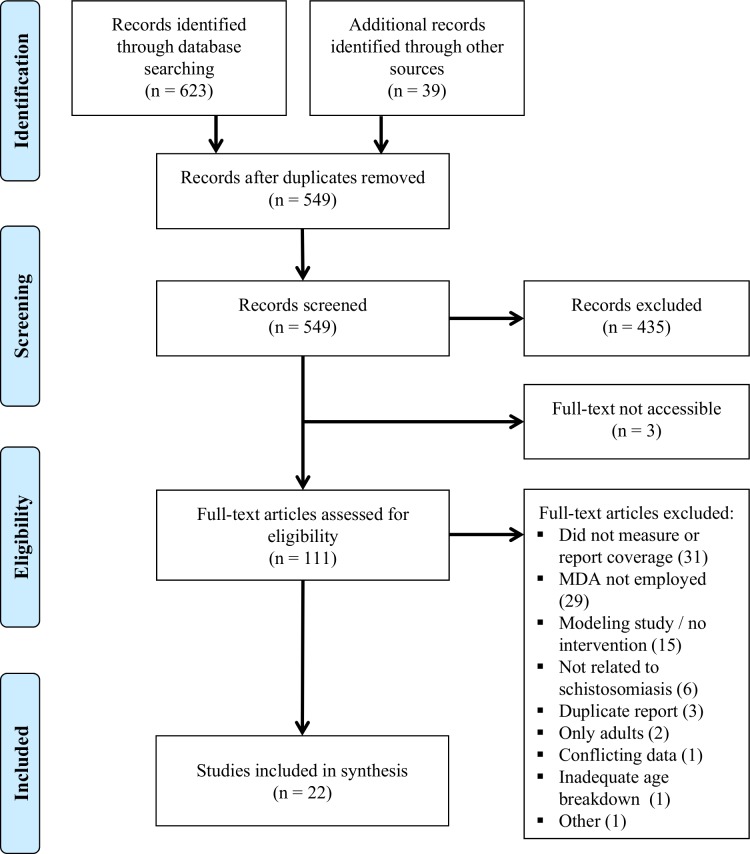
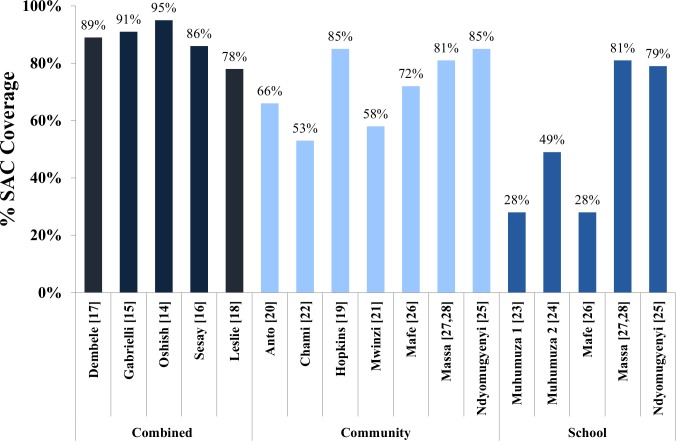
Methodology/principal findings: This review was registered prospectively with PROSPERO (CRD 42015017656). Five hundred forty-nine publication of potential relevance were identified through database searches, reference lists, and personal communications. Eligible studies included those published before October 2015, written in English or French, containing quantitative or qualitative data about coverage rates for MDA of school-aged children with praziquantel. Among the 22 selected studies, combined community- and school-based programs achieved the highest median coverage rates (89%), followed by community-based programs (72%). School-based programs had both the lowest median coverage of children overall (49%) and the lowest coverage of the non-enrolled subpopulation of children. Qualitatively, major factors affecting program success included fear of side effects, inadequate education about schistosomiasis, lack of incentives for drug distributors, and inequitable distribution to minority groups.
Conclusions/significance: This review provides an evidence-based framework for the development of future schistosomiasis control programs. Based on our results, a combined community and school-based delivery system should maximize coverage for both in- and out-of-school children, especially when combined with interventions such as snacks for treated children, educational campaigns, incentives for drug distributors, and active inclusion of marginalized groups.
Trial registration: ClinicalTrials.gov CRD42015017656.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Ezeamama AE, He CL, Shen Y, Yin XP, Binder SC, Campbell CH Jr., et al. Gaining and sustaining schistosomiasis control: study protocol and baseline data prior to different treatment strategies in five African countries. BMC Infect Dis. 2016;16(1):229 doi: 10.1186/s12879-016-1575-2 - DOI - PMC - PubMed
-
- Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. 2014;383(9936):2253–2264. doi: 10.1016/S0140-6736(13)61949-2 - DOI - PMC - PubMed
-
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. doi: 10.1016/S0140-6736(15)60692-4 - DOI - PMC - PubMed
-
- WHO. Schistosomiasis and soil-transmitted helminthiases: number of people treated in 2015. Wkly Epidemiol Rec. 2016;91(49–50):585–595. - PubMed
-
- King CH, Bertsch D. Historical perspective: snail control to prevent schistosomiasis. PLoS Negl Trop Dis. 2015;9(4):e0003657 doi: 10.1371/journal.pntd.0003657 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
