

Some Clinically Useful Information that Neuropsychology Provides Patients, Carepartners, Neurologists, and Neurosurgeons About Deep Brain Stimulation for Parkinson's Disease
- PMID: 29077802
- PMCID: PMC5860398
- DOI: 10.1093/arclin/acx090
Some Clinically Useful Information that Neuropsychology Provides Patients, Carepartners, Neurologists, and Neurosurgeons About Deep Brain Stimulation for Parkinson's Disease
Abstract
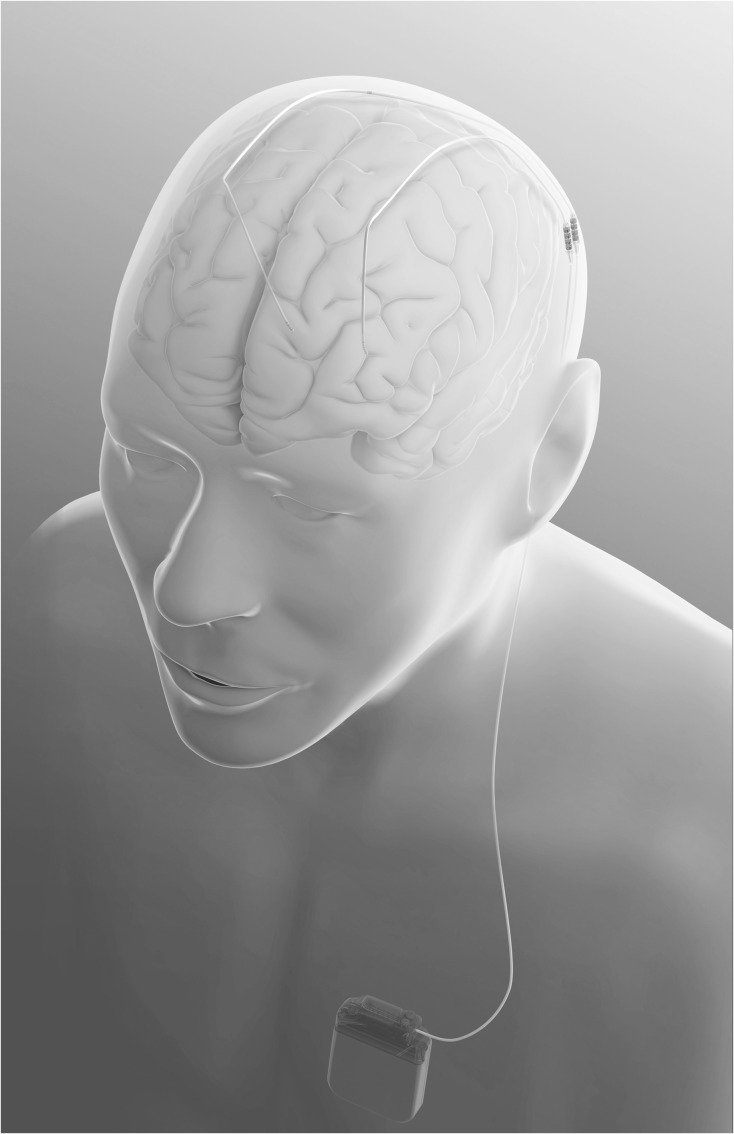
Deep brain stimulation (DBS) is an effective (but non-curative) treatment for some of the motor symptoms and treatment complications associated with dopaminergic agents in Parkinson's disease (PD). DBS can be done relatively safely and is associated with quality of life gains. In most DBS centers, neuropsychological evaluations are performed routinely before surgery, and sometimes after surgery. The purpose of such evaluation is not to decide solely on its results whether or not to offer DBS to a given candidate, but to provide the patient and treatment team with the best available information to make reasonable risk-benefit assessments. This review provides information relevant to the questions often asked by patients and their carepartners, neurologists, and neurosurgeons about neuropsychological outcomes of DBS, including neuropsychological adverse event rates, magnitude of cognitive changes, outcomes after unilateral versus bilateral surgery directed at various targets, impact of mild cognitive impairment (MCI) on outcome, factors implicated in neurobehavioral outcomes, and safety of newer interventions or techniques such as asleep surgery and current steering.
Keywords: Anxiety; Cognition; Deep brain stimulation; Depression; Impulsiveness; Mild cognitive impairment (MCI); Neuromodulation; Neuropsychology; Parkinson's disease; Psychosis; Quality of life.
© The Author 2017. Published by Oxford University Press.
Figures
References
-
- Abboud H., Floden D., Thompson N. R., Genc G., Oravivattanakul S., Alsallom F., et al. (2015). Impact of mild cognitive impairment on outcome following deep brain stimulation surgery for Parkinson's disease. Parkinsonism & Related Disorders, 21, 249–253. doi:10.1016/j.parkreldis.2014.12.018. - DOI - PubMed
-
- Abboud H., Mehanna R., Machado A., Ahmed A., Gostkowski M., Cooper S., et al. (2014). Comprehensive, multidisciplinary deep brain stimulation screenig for Parkinson patients: no room for “short cuts”. Movement Disorders: Clinical Practice, 1 (4), 336–341. doi:10.1002/mdc3.12090. - DOI - PMC - PubMed
-
- Anderson V. C., Burchiel K. J., Hogarth P., Favre J., & Hammerstad J. P. (2005). Pallidal vs subthalamic nucleus deep brain stimulation in Parkinson disease. Archives of Neurology, 62, 554–560. - PubMed
-
- Appleby B. S., Duggan P. S., Regenberg A., & Rabins P. V. (2007). Psychiatric and neuropsychiatric adverse events associated with deep brain stimulation: a meta-analysis of ten years’ experience. Movement Disorders, 22, 1722–1728. doi:10.1002/mds.21551. - DOI - PubMed
-
- Aybek S., Gronchi-Perrin A., Berney A., Chiuve S. C., Villemure J. G., Burkhard P. R., et al. (2007). Long-term cognitive profile and incidence of dementia after STN-DBS in Parkinson's disease. Movement Disorders, 22, 974–981. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
