

Genomic analysis of the origins and evolution of multicentric diffuse lower-grade gliomas
- PMID: 29077933
- PMCID: PMC5892142
- DOI: 10.1093/neuonc/nox205
Genomic analysis of the origins and evolution of multicentric diffuse lower-grade gliomas
Abstract
Background: Rare multicentric lower-grade gliomas (LGGs) represent a unique opportunity to study the heterogeneity among distinct tumor foci in a single patient and to infer their origins and parallel patterns of evolution.
Methods: In this study, we integrate clinical features, histology, and immunohistochemistry for 4 patients with multicentric LGG, arising both synchronously and metachronously. For 3 patients we analyze the phylogeny of the lesions using exome sequencing, including one case with a total of 8 samples from the 2 lesions.
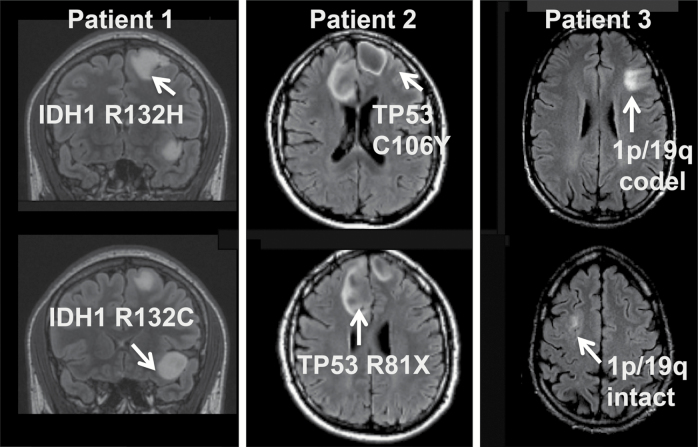
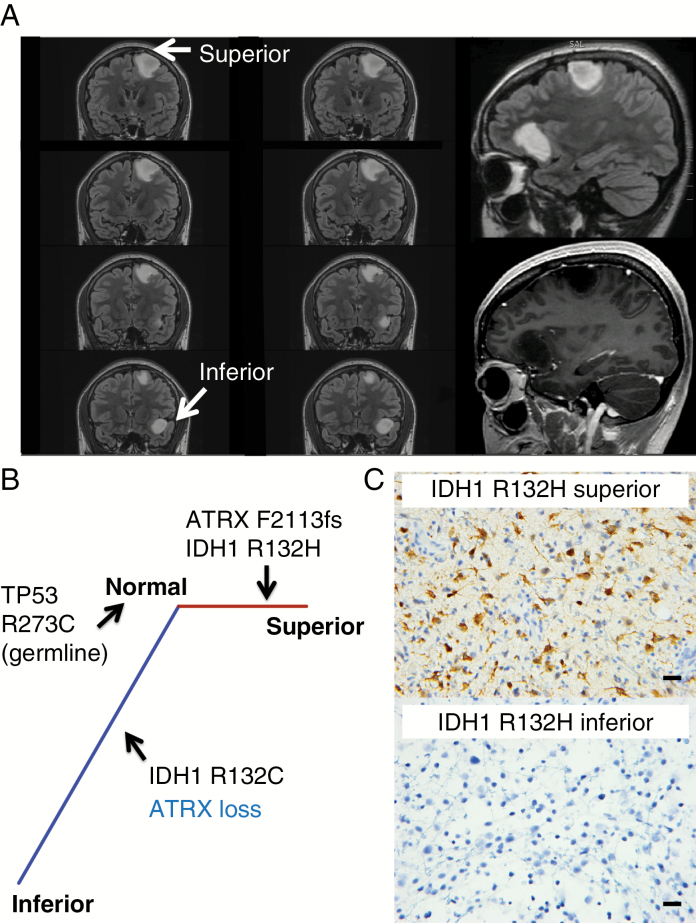
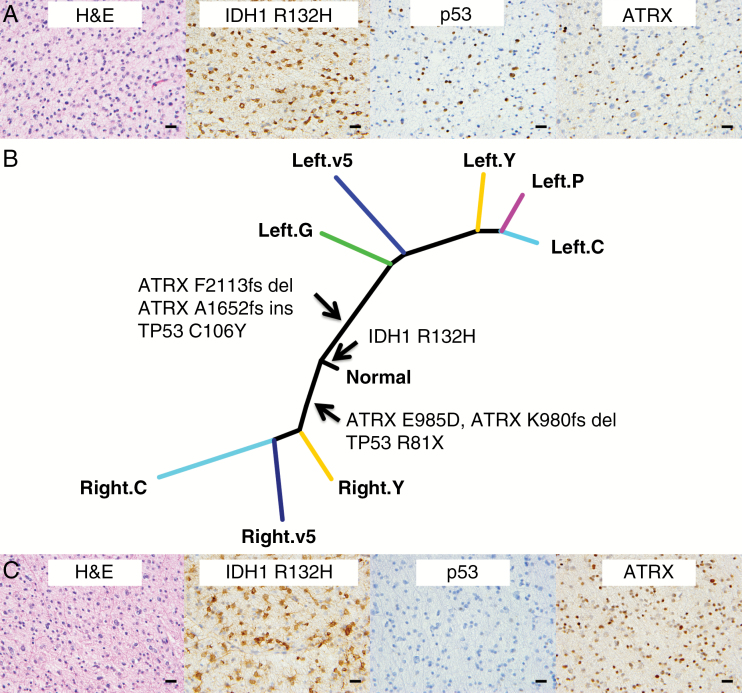
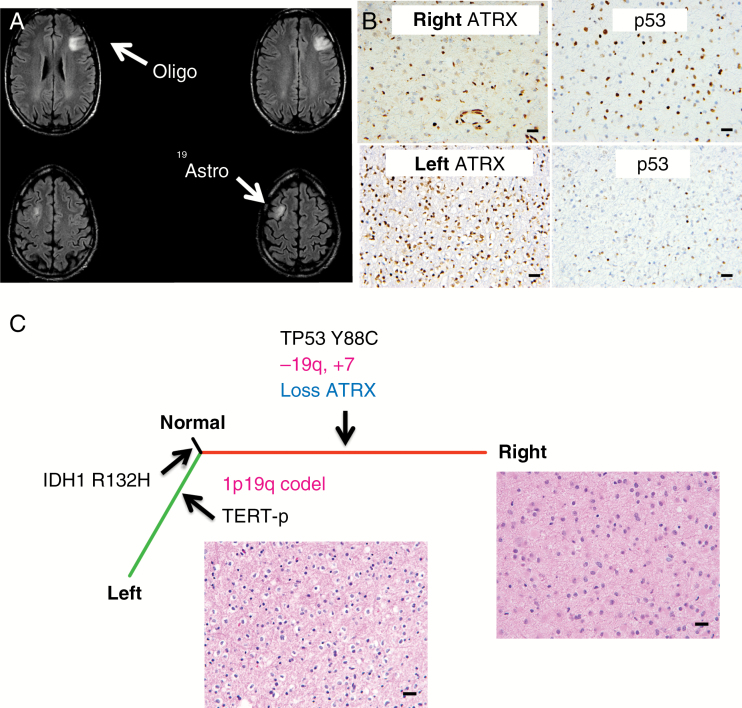
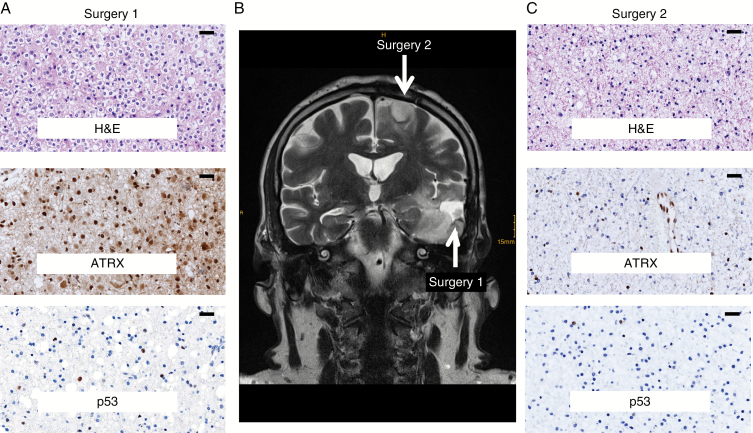
Results: One patient was diagnosed with multicentric isocitrate dehydrogenase 1 (IDH1) mutated diffuse astrocytomas harboring distinct IDH1 mutations, R132H and R132C; the latter mutation has been associated with Li-Fraumeni syndrome, which was subsequently confirmed in the patient's germline DNA and shown in additional cases with The Cancer Genome Atlas data. In another patient, phylogenetic analysis of synchronously arising grade II and grade III diffuse astrocytomas demonstrated a single shared mutation, IDH1 R132H, and revealed convergent evolution via non-overlapping mutations in ATRX and TP53. In 2 cases, there was divergent evolution of IDH1-mutated and 1p/19q-codeleted oligodendroglioma and IDH1-mutated and 1p/19q-intact diffuse astrocytoma, occurring synchronously in one case and metachronously in a second.
Conclusions: Each tumor in multicentric LGG cases may arise independently or may diverge very early in their development, presenting as genetically and histologically distinct tumors. Comprehensive sampling of these lesions can therefore significantly alter diagnosis and management. Additionally, somatic IDH1 R132C mutation in either multicentric or solitary LGG identifies unsuspected germline TP53 mutation, validating the limited number of published cases.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK.. WHO Classification of Tumours of the Central Nervous System. 4 ed Lyon: International Agency for Research on Cancer; 2016.
-
- Suzuki H, Aoki K, Chiba K et al. Mutational landscape and clonal architecture in grade II and III gliomas. Nat Genet. 2015;47(5):458–468. - PubMed
-
- Louis DN, Perry A, Reifenberger G et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
