

Safety and efficacy of combined resection of colorectal peritoneal and liver metastases
- PMID: 29078882
- PMCID: PMC5663460
- DOI: 10.1016/j.jss.2017.05.126
Safety and efficacy of combined resection of colorectal peritoneal and liver metastases
Abstract
Background: To determine if a select subgroup of patients with combined liver and peritoneal colorectal metastases would derive oncologic benefit from surgical resection as a component of multimodality treatment.
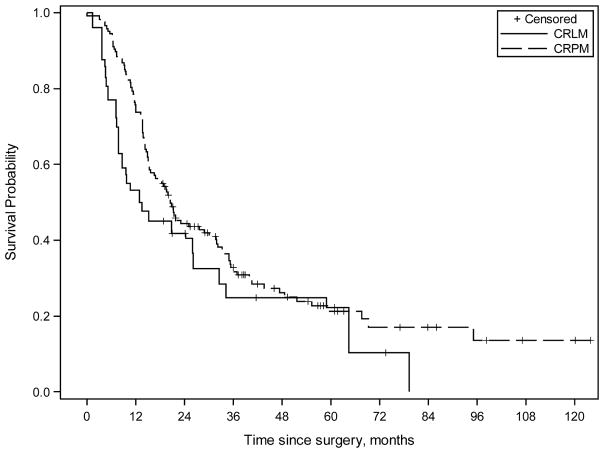
Materials and methods: We retrospectively compared 32 patients with combined colorectal peritoneal and liver metastases (CRLM) and 173 patients with peritoneal metastases only (CRPM) undergoing cytoreductive surgery with hyperthermic intraperitoneal chemoperfusion (CRS-HIPEC). Kaplan-Meier survival curves and multivariate Cox-regression models identified prognostic factors affecting survival.
Results: Major postoperative complications (Clavien-Dindo grades 3-5) occurred in 32% (CRLM) and 17% (CRPM) of patients (P = 0.08). After an estimated median follow-up from surgery of 57 mo, propensity score-adjusted median progression-free survival was 5.1 mo (CRLM) and 7.6 mo (CRPM), whereas median overall survival was 13 mo (CRLM) and 21 mo (CRPM). Multivariate Cox-regression analysis of the CRLM group identified number of liver metastases to be the only independent predictor of poor survival (hazard ratio: 2.3, P = 0.03), with a dramatic decrease in survival in patients with more than three liver metastases.
Conclusions: Simultaneous resection of colorectal liver metastases at the time of cytoreductive surgery with hyperthermic intraperitoneal chemoperfusion for peritoneal metastases may be associated with worse survival, especially in patients with more than three liver metastases.
Keywords: Colorectal cancer; Cytoreductive surgery; HIPEC; Metastases.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures



References
-
- Elias D, Honore C, Dumont F, Ducreux M, Boige V, Malka D, et al. Results of systematic second-look surgery plus HIPEC in asymptomatic patients presenting a high risk of developing colorectal peritoneal carcinomatosis. Annals of surgery. 2011;254(2):289–93. doi: 10.1097/SLA.0b013e31822638f6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
