

2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups
- PMID: 29079590
- PMCID: PMC5736307
- DOI: 10.1136/annrheumdis-2017-211468
2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups
Erratum in
-
Correction: European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups.Ann Rheum Dis. 2018 Sep;77(9):e64. doi: 10.1136/annrheumdis-2017-211468corr1. Ann Rheum Dis. 2018. PMID: 30097512 No abstract available.
Abstract
Objective: To develop and validate new classification criteria for adult and juvenile idiopathic inflammatory myopathies (IIM) and their major subgroups.
Methods: Candidate variables were assembled from published criteria and expert opinion using consensus methodology. Data were collected from 47 rheumatology, dermatology, neurology and paediatric clinics worldwide. Several statistical methods were used to derive the classification criteria.
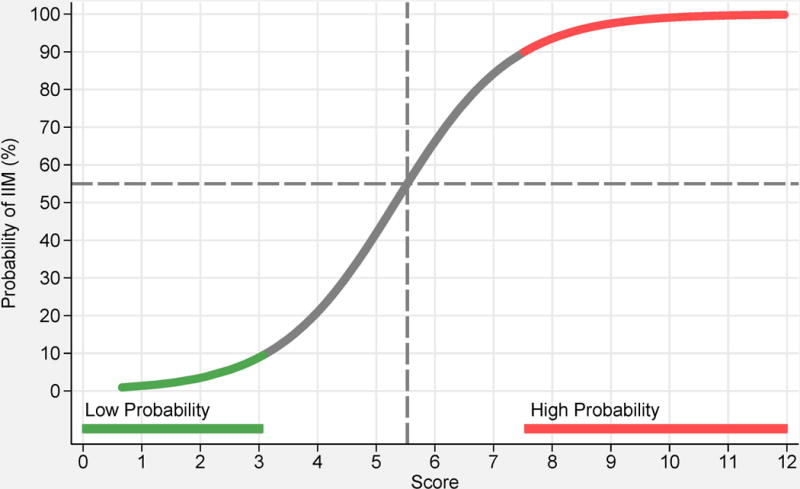
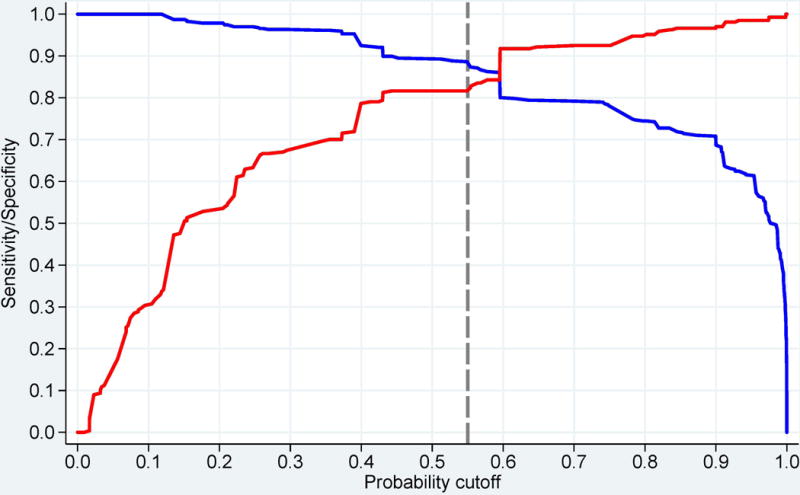
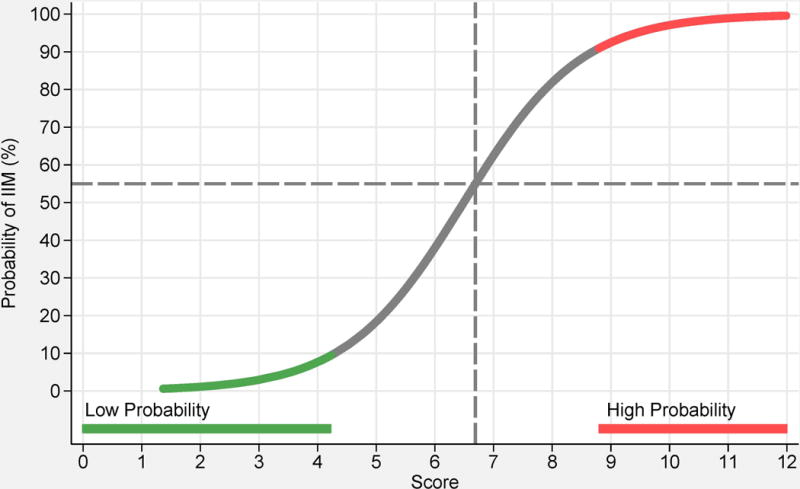
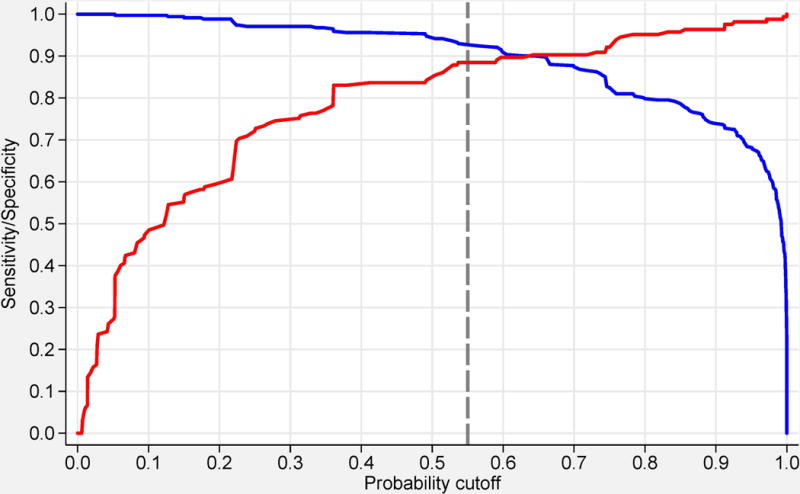
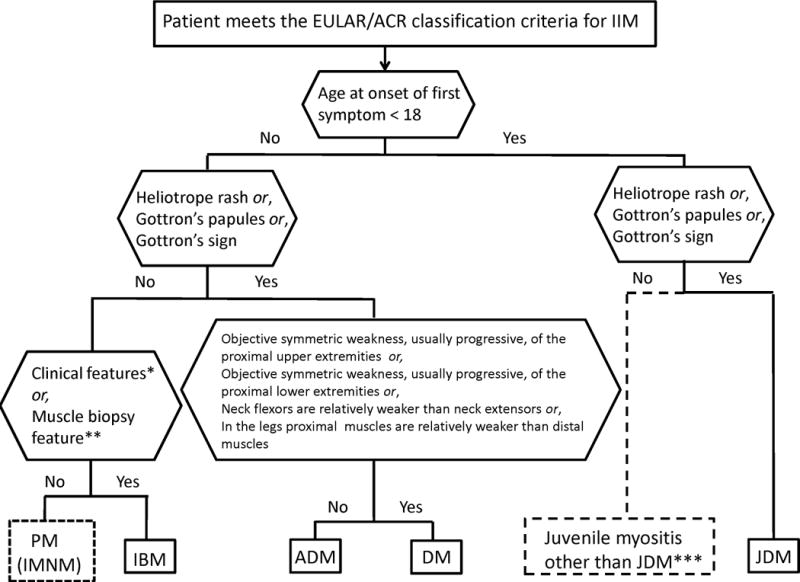
Results: Based on data from 976 IIM patients (74% adults; 26% children) and 624 non-IIM patients with mimicking conditions (82% adults; 18% children), new criteria were derived. Each item is assigned a weighted score. The total score corresponds to a probability of having IIM. Subclassification is performed using a classification tree. A probability cut-off of 55%, corresponding to a score of 5.5 (6.7 with muscle biopsy) 'probable IIM', had best sensitivity/specificity (87%/82% without biopsies, 93%/88% with biopsies) and is recommended as a minimum to classify a patient as having IIM. A probability of ≥90%, corresponding to a score of ≥7.5 (≥8.7 with muscle biopsy), corresponds to 'definite IIM'. A probability of <50%, corresponding to a score of <5.3 (<6.5 with muscle biopsy), rules out IIM, leaving a probability of ≥50 to <55% as 'possible IIM'.
Conclusions: The European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) classification criteria for IIM have been endorsed by international rheumatology, dermatology, neurology and paediatric groups. They employ easily accessible and operationally defined elements, and have been partially validated. They allow classification of 'definite', 'probable' and 'possible' IIM, in addition to the major subgroups of IIM, including juvenile IIM. They generally perform better than existing criteria.
Keywords: autoimmune diseases; dermatomyositis; polymyositis.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JAS has received research grants from Takeda and Savient and consultant fees from Savient, Takeda, Regeneron, Merz, Iroko, Bioiberica, Crealta and Allergan. JAS serves as the principal investigator for an investigator-initiated study funded by Horizon pharmaceuticals through a grant to DINORA, Inc., a 501 (c)(3) entity. JAS is a member of the executive committee of OMERACT, an organisation that develops outcome measures in rheumatology and receives arms-length funding from 36 companies; a member of the American College of Rheumatology’s (ACR) Annual Meeting Planning Committee (AMPC); Chair of the ACR Meet-the-Professor, Workshop and Study Group Subcommittee; and a member of the Veterans Affairs Rheumatology Field Advisory Committee. HC and RGC’s work in myositis is partly funded by grants from Arthritis Research UK (18474) and the Medical Research Council (MR/N003322/1). JV’s work in myositis is supported by Project (Ministry of Health, Czech Republic) for conceptual development of research organization 00023728.
Figures
Comment in
-
2017 EULAR/ACR classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups: little emphasis on autoantibodies, why?Ann Rheum Dis. 2018 Nov;77(11):e77. doi: 10.1136/annrheumdis-2017-212701. Epub 2017 Nov 23. Ann Rheum Dis. 2018. PMID: 29170201 No abstract available.
-
Response to: '2017 EULAR/ACR classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups: little emphasis on autoantibodies, why?' by Malaviya.Ann Rheum Dis. 2018 Nov;77(11):e78. doi: 10.1136/annrheumdis-2017-212709. Epub 2017 Dec 15. Ann Rheum Dis. 2018. PMID: 29247124 No abstract available.
-
Detection of myositis-specific antibodies.Ann Rheum Dis. 2019 Jan;78(1):e7. doi: 10.1136/annrheumdis-2017-212915. Epub 2018 Jan 25. Ann Rheum Dis. 2019. PMID: 29371203 No abstract available.
-
Response to: 'Detection of myositis-specific antibodies' by Vulsteke et al.Ann Rheum Dis. 2019 Jan;78(1):e8. doi: 10.1136/annrheumdis-2018-212948. Epub 2018 Jan 30. Ann Rheum Dis. 2019. PMID: 29382639 No abstract available.
-
Reply.Arthritis Rheumatol. 2018 Jun;70(6):976. doi: 10.1002/art.40473. Epub 2018 May 2. Arthritis Rheumatol. 2018. PMID: 29513922 No abstract available.
-
Consideration of Antisynthetase Syndrome Features in Classifying Patients as Having Idiopathic Inflammatory Myopathy: Comment on the Article by Lundberg et al.Arthritis Rheumatol. 2018 Jun;70(6):975-976. doi: 10.1002/art.40478. Epub 2018 Apr 29. Arthritis Rheumatol. 2018. PMID: 29513937 No abstract available.
-
Detection of myositis-specific antibodies: additional notes.Ann Rheum Dis. 2019 Apr;78(4):e29. doi: 10.1136/annrheumdis-2018-213320. Epub 2018 Mar 13. Ann Rheum Dis. 2019. PMID: 29535123 No abstract available.
-
Time to personalize the treatment of anti-MDA-5 associated lung disease.Ann Rheum Dis. 2019 Jun;78(6):e52. doi: 10.1136/annrheumdis-2018-213285. Epub 2018 Apr 11. Ann Rheum Dis. 2019. PMID: 29643107 No abstract available.
-
Response to: 'Time to personalise the treatment of anti-MDA-5 associated lung disease' by Lake et al.Ann Rheum Dis. 2019 Jun;78(6):e53. doi: 10.1136/annrheumdis-2018-213519. Epub 2018 May 3. Ann Rheum Dis. 2019. PMID: 29724727 No abstract available.
References
-
- Plotz PH, Rider GL, Targoff IN, et al. NIH conference. Myositis: immunologic contributions to understanding cause, pathogenesis, and therapy. Ann Intern Med. 1995;122:715–24. - PubMed
-
- Dalakas MC. Inflammatory muscle diseases. N Eng J Med. 2015;372:1734–47. - PubMed
-
- Rider LG, Giannini EH, Brunner HI, et al. International Myositis Assessment and Clinical Studies Group. International consensus on preliminary definitions of improvement in adult and juvenile myositis. Arthritis Rheum. 2004;50:2281–90. - PubMed
-
- Oddis CV, Rider LG, Reed AM, et al. International consensus guidelines for trials of therapies in the idiopathic inflammatory myopathies. Arthritis Rheum. 2005;52:2607–15. - PubMed
-
- Medsger TA, Jr, Dawson WN, Jr, Masi AT. The epidemiology of polymyositis. Am J Med. 1970;48:715–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
