

Individual Trade-Offs Between Possible Benefits and Risks of Cancer Treatments: Results from a Stated Preference Study with Patients with Multiple Myeloma
- PMID: 29079638
- PMCID: PMC5759823
- DOI: 10.1634/theoncologist.2017-0257
Individual Trade-Offs Between Possible Benefits and Risks of Cancer Treatments: Results from a Stated Preference Study with Patients with Multiple Myeloma
Abstract
Background: The objectives of this study were to elicit the preferences of patients with multiple myeloma regarding the possible benefits and risks of cancer treatments and to illustrate how such data may be used to estimate patients' acceptance of new treatments.
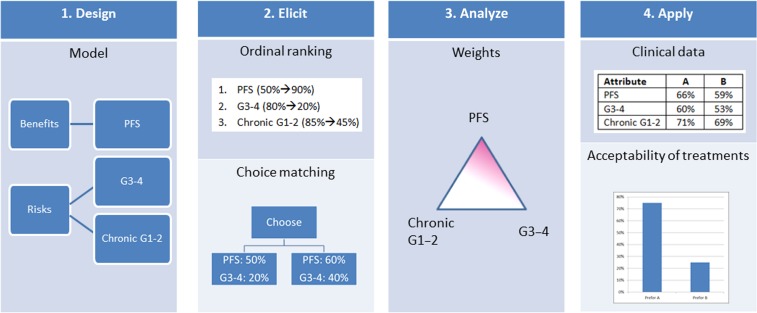
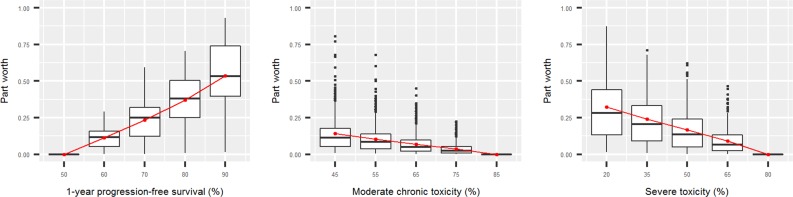
Patients and methods: Patients with multiple myeloma from the cancer charity Myeloma UK were invited to participate in an online survey based on multicriteria decision analysis and swing weighting to elicit individual stated preferences for the following attributes: (a) 1-year progression-free survival (PFS, ranging from 50% to 90%), (b) mild or moderate toxicity for 2 months or longer (ranging from 85% to 45%), and (c) severe or life-threatening toxicity (ranging from 80% to 20%).
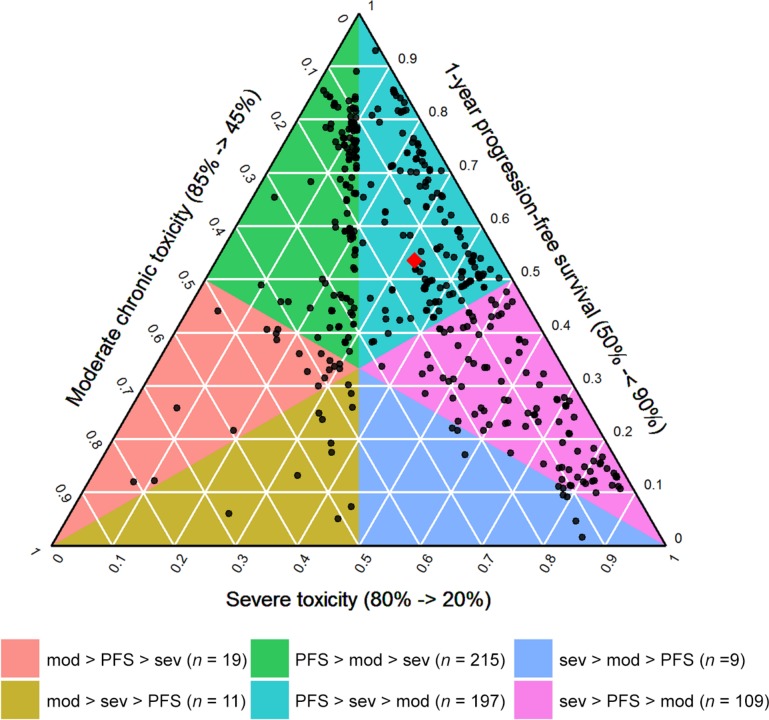
Results: A total of 560 participants completed the survey. The average weight given to PFS was 0.54, followed by 0.32 for severe or life-threatening toxicity and 0.14 for mild or moderate chronic toxicity. Participants who ranked severe or life-threatening toxicity above mild or moderate chronic toxicity (56%) were more frequently younger, working, and looking after dependent family members and had more frequently experienced severe or life-threatening side effects. The amount of weight given to PFS did not depend on any of the collected covariates. The feasibility of using the collected preference data to estimate the patients' acceptance of specific multiple myeloma treatments was demonstrated in a subsequent decision analysis example.
Conclusion: Stated preference studies provide a systematic approach to gain knowledge about the distribution of preferences in the population and about what this implies for patients' acceptance of specific treatments.
Implications for practice: This study demonstrated how quantitative preference statements from a large group of participants can be collected through an online survey and how such information may be used to explore the acceptability of specific treatments based on the attributes studied. Results from such studies have the potential to become an important new tool for gathering patient views and studying heterogeneity in preferences in a systematic way, along with other methods, such as focus groups and expert opinions.
Keywords: Benefit‐risk assessment; Multicriteria decision analysis; Patient preferences; Regulatory science.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Medical Device Innovation Consortium . Medical device innovation consortium (MDIC) patient centered benefit‐risk project report: A framework for incorporating information on patient preferences regarding benefit and risk into regulatory assessments of new medical technology. Available at http://mdic.org/wp-content/uploads/2015/05/MDIC_PCBR_Framework_Web1.pdf. Accessed May 24, 2017.
-
- European Medicines Agency . Revised framework for interaction between the European Medicines Agency and patients and consumers and their organisations. October 16, 2014. Available at http://www.ema.europa.eu/docs/en_GB/document_library/Other/2009/12/WC500.... Accessed May 24, 2017.
-
- Postmus D, Mavris M, Hillege HL et al. Incorporating patient preferences into drug development and regulatory decision making: Results from a quantitative pilot study with cancer patients, carers, and regulators. Clin Pharmacol Ther 2016;99:548–554. - PubMed
-
- Tervonen T, van Valkenhoef G, Buskens E et al. A stochastic multicriteria model for evidence‐based decision making in drug benefit‐risk analysis. Stat Med 2011;30:1419–1428. - PubMed
-
- Moreau P, Masszi T, Grzasko N et al. Oral Ixazomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med 2016;374:1621–1634. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
