

Experimental imaging in orthotopic renal cell carcinoma xenograft models: comparative evaluation of high-resolution 3D ultrasonography, in-vivo micro-CT and 9.4T MRI
- PMID: 29079842
- PMCID: PMC5660163
- DOI: 10.1038/s41598-017-14759-1
Experimental imaging in orthotopic renal cell carcinoma xenograft models: comparative evaluation of high-resolution 3D ultrasonography, in-vivo micro-CT and 9.4T MRI
Abstract
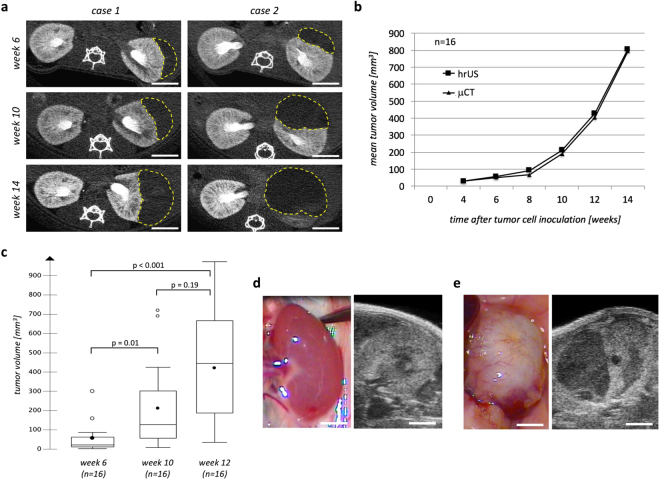
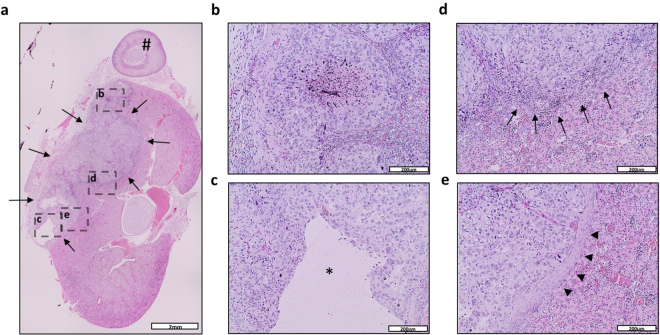
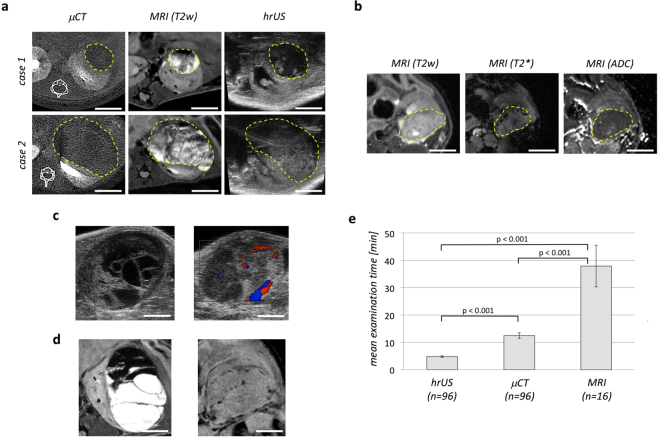
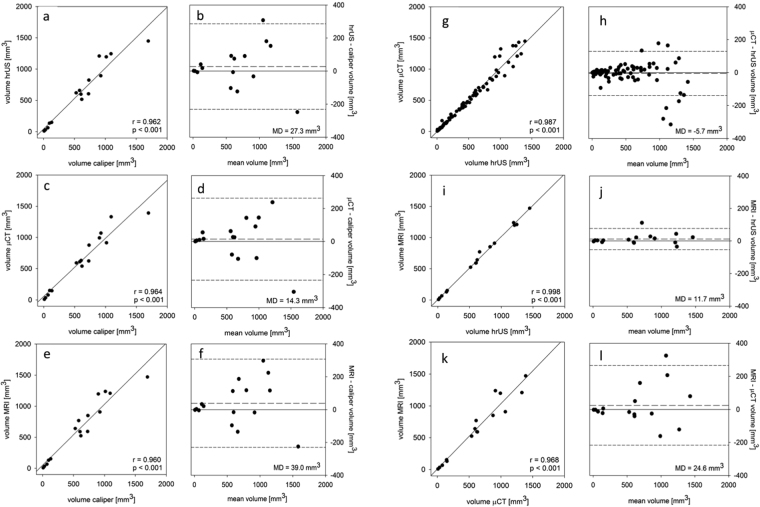
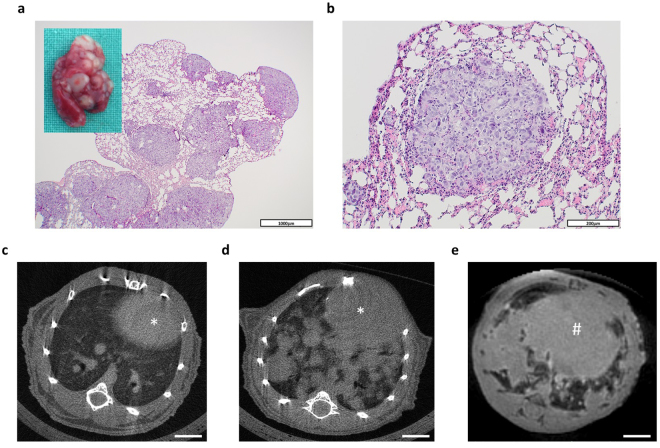
In this study, we aimed to comparatively evaluate high-resolution 3D ultrasonography (hrUS), in-vivo micro-CT (μCT) and 9.4T MRI for the monitoring of tumor growth in an orthotopic renal cell carcinoma (RCC) xenograft model since there is a lack of validated, non-invasive imaging tools for this purpose. 1 × 106 Caki-2 RCC cells were implanted under the renal capsule of 16 immunodeficient mice. Local and systemic tumor growth were monitored by regular hrUS, μCT and MRI examinations. Cells engrafted in all mice and gave rise to exponentially growing, solid tumors. All imaging techniques allowed to detect orthotopic tumors and to precisely calculate their volumes. While tumors appeared homogenously radiolucent in μCT, hrUS and MRI allowed for a better visualization of intratumoral structures and surrounding soft tissue. Examination time was the shortest for hrUS, followed by μCT and MRI. Tumor volumes determined by hrUS, μCT and MRI showed a very good correlation with each other and with caliper measurements at autopsy. 10 animals developed pulmonary metastases being well detectable by μCT and MRI. In conclusion, each technique has specific strengths and weaknesses, so the one(s) best suitable for a specific experiment may be chosen individually.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
