

Classification of Cough as a Symptom in Adults and Management Algorithms: CHEST Guideline and Expert Panel Report
- PMID: 29080708
- PMCID: PMC6689094
- DOI: 10.1016/j.chest.2017.10.016
Classification of Cough as a Symptom in Adults and Management Algorithms: CHEST Guideline and Expert Panel Report
Abstract
Background: We performed systematic reviews using the population, intervention, comparison, outcome (PICO) format to answer the following key clinical question: Are the CHEST 2006 classifications of acute, subacute and chronic cough and associated management algorithms in adults that were based on durations of cough useful?
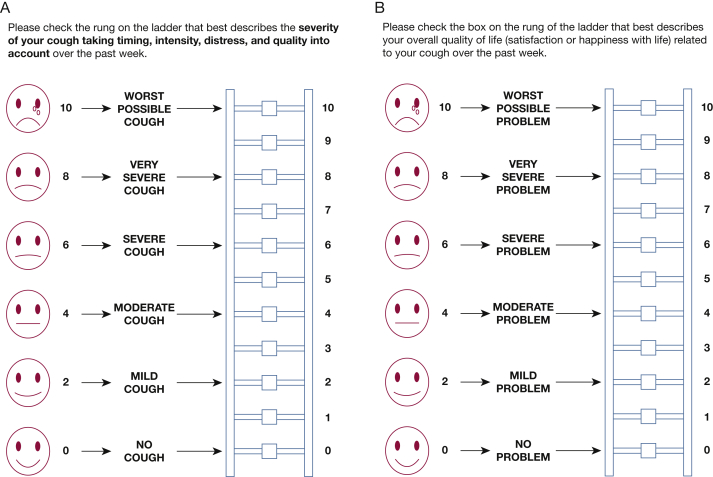
Methods: We used the CHEST Expert Cough Panel's protocol for the systematic reviews and the American College of Chest Physicians (CHEST) methodological guidelines and Grading of Recommendations Assessment, Development, and Evaluation framework. Data from the systematic reviews in conjunction with patient values and preferences and the clinical context were used to form recommendations or suggestions. Delphi methodology was used to obtain the final grading.
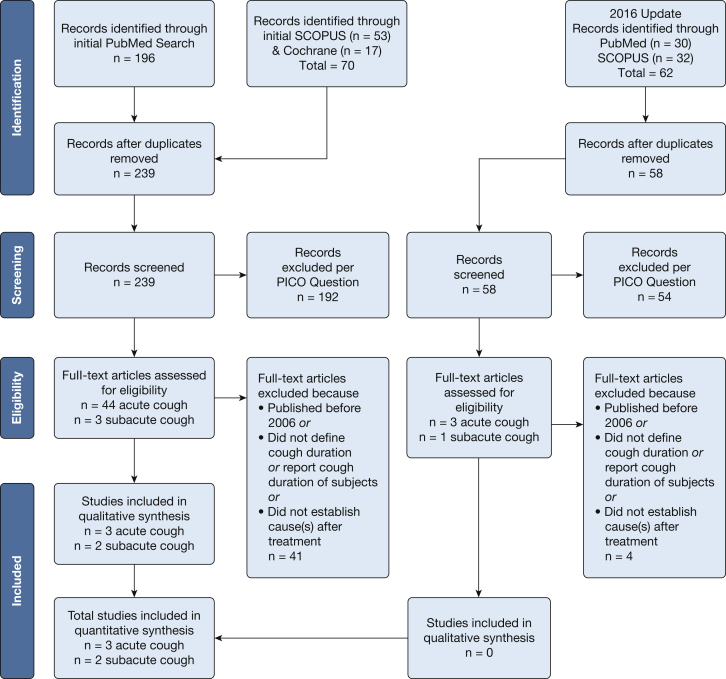
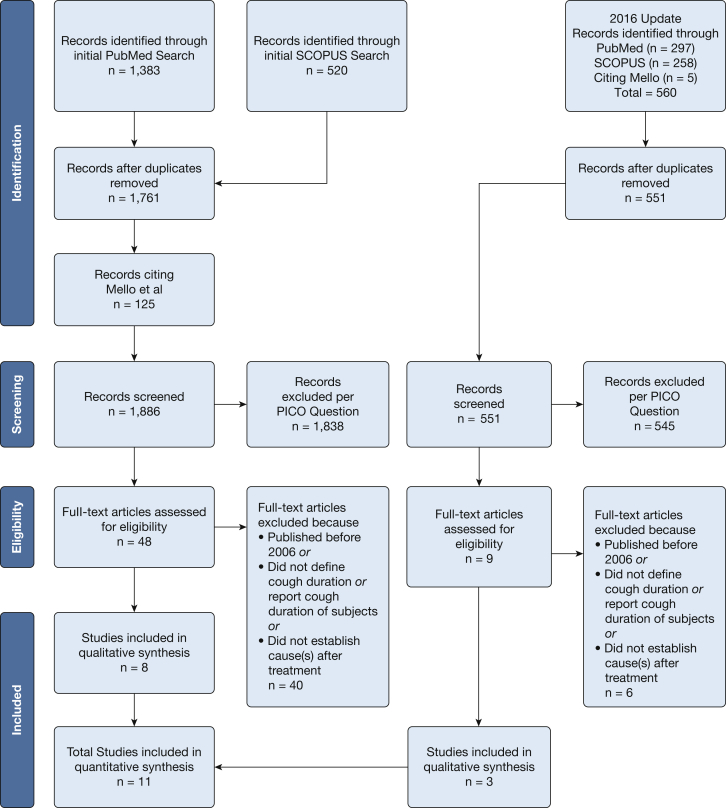
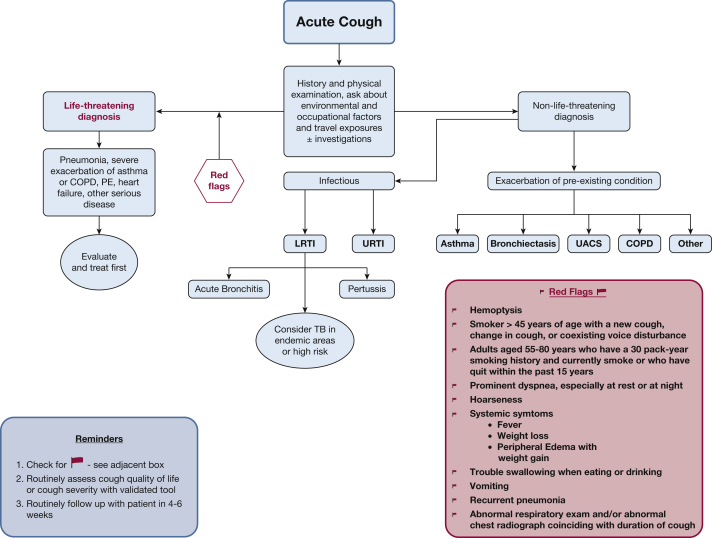
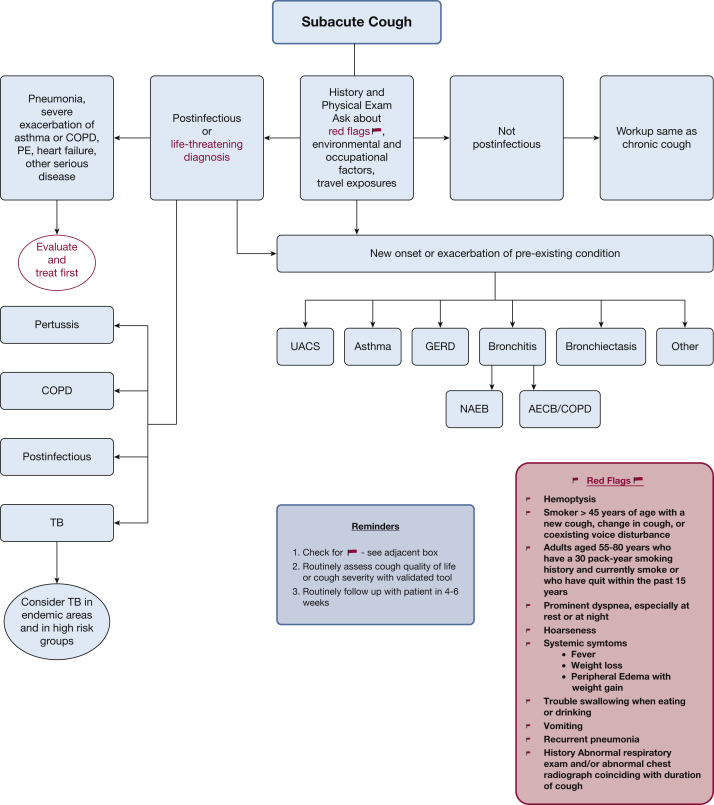
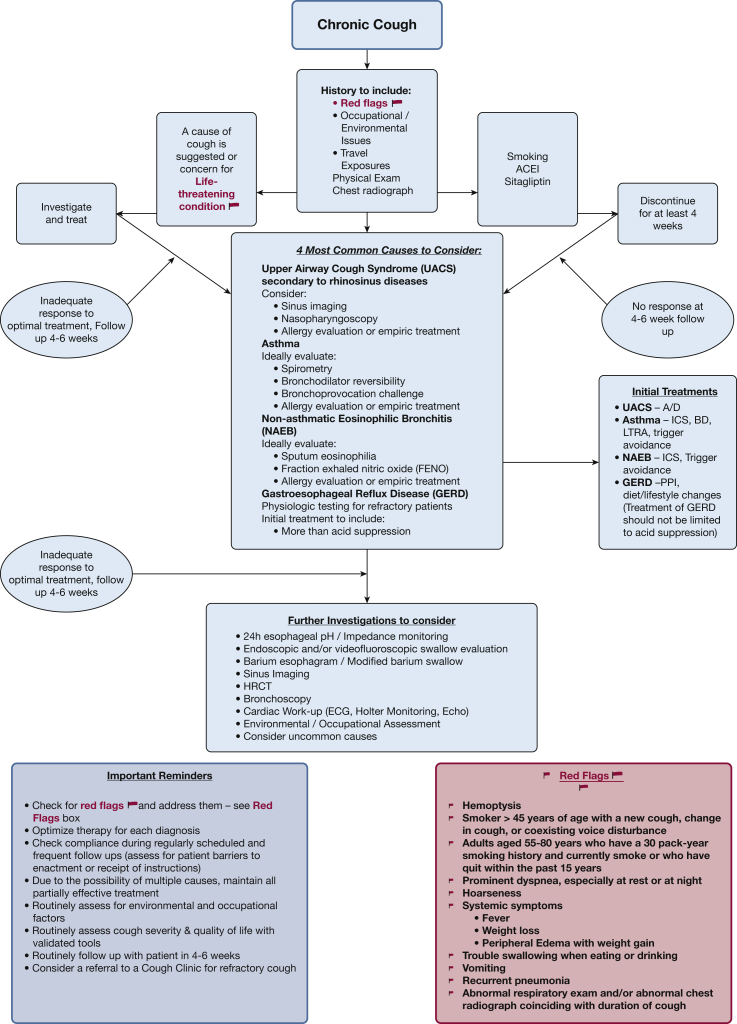
Results: With respect to acute cough (< 3 weeks), only three studies met our criteria for quality assessment, and all had a high risk of bias. As predicted by the 2006 CHEST Cough Guidelines, the most common causes were respiratory infections, most likely of viral cause, followed by exacerbations of underlying diseases such as asthma and COPD and pneumonia. The subjects resided on three continents: North America, Europe, and Asia. With respect to subacute cough (duration, 3-8 weeks), only two studies met our criteria for quality assessment, and both had a high risk of bias. As predicted by the 2006 guidelines, the most common causes were postinfectious cough and exacerbation of underlying diseases such as asthma, COPD, and upper airway cough syndrome (UACS). The subjects resided in countries in Asia. With respect to chronic cough (> 8 weeks), 11 studies met our criteria for quality assessment, and all had a high risk of bias. As predicted by the 2006 guidelines, the most common causes were UACS from rhinosinus conditions, asthma, gastroesophageal reflux disease, nonasthmatic eosinophilic bronchitis, combinations of these four conditions, and, less commonly, a variety of miscellaneous conditions and atopic cough in Asian countries. The subjects resided on four continents: North America, South America, Europe, and Asia.
Conclusions: Although the quality of evidence was low, the published literature since 2006 suggests that CHEST's 2006 Cough Guidelines and management algorithms for acute, subacute, and chronic cough in adults appeared useful in diagnosing and treating patients with cough around the globe. These same algorithms have been updated to reflect the advances in cough management as of 2017.
Keywords: cough; evidence-based medicine; guidelines; management algorithms for acute, subacute, and chronic cough in adults.
Copyright © 2017 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Mello C.J., Irwin R.S., Curley F.J. Predictive values of the character, timing, and complications of chronic cough in diagnosing its cause. Arch Intern Med. 1996;156(9):997–1003. - PubMed
-
- Irwin R.S., Boulet L.P., Cloutier M.M. Managing cough as a defense mechanism and as a symptom. A consensus panel report of the American College of Chest Physicians. Chest. 1998;114(2 suppl Managing):133S–181S. - PubMed
-
- Pratter M.R., Brightling C.E., Boulet L.P. An empiric integrative approach to the management of cough: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1 suppl):222S–231S. - PubMed
-
- Lewis S.Z., Diekemper R., Ornelas J. Methodologies for the development of CHEST guidelines and expert panel reports. Chest. 2014;146(1):182–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
