

Impact of pain and postoperative complications on patient-reported outcome measures 5 years after microvascular decompression or partial sensory rhizotomy for trigeminal neuralgia
- PMID: 29080911
- PMCID: PMC5735194
- DOI: 10.1007/s00701-017-3350-6
Impact of pain and postoperative complications on patient-reported outcome measures 5 years after microvascular decompression or partial sensory rhizotomy for trigeminal neuralgia
Abstract
Background: Microvascular decompression (MVD) and partial sensory rhizotomy (PSR) provide longstanding pain relief in trigeminal neuralgia (TN). Given their invasiveness, complications can result from such posterior fossa procedures, but the impact of these procedures and their complications on patient-reported outcome measures (PROM), such as quality of life and distress, are not well established.
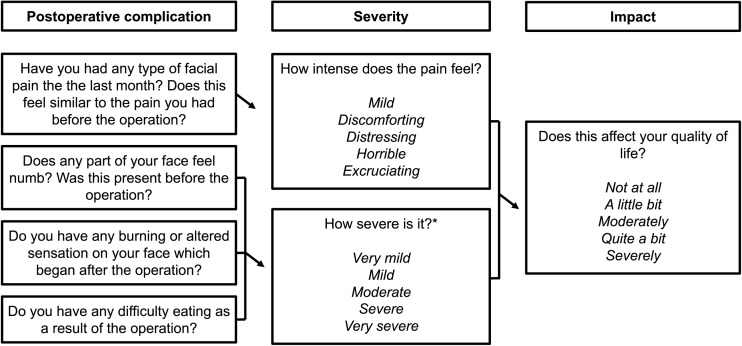
Method: Five years after surgery, patients who underwent first MVD or PSR for TN at one institution, between 1982 and 2002, were sent a self-completion assessment set containing a range of PROMs: the Short Form-12 (SF-12) questionnaire to assess quality of life, the Hospital Anxiety and Depression Scale (HADS) to assess distress, and a questionnaire containing questions about postoperative complications, their severity and impact on quality of life. These findings and demographic data were compared between MVD and PSR.
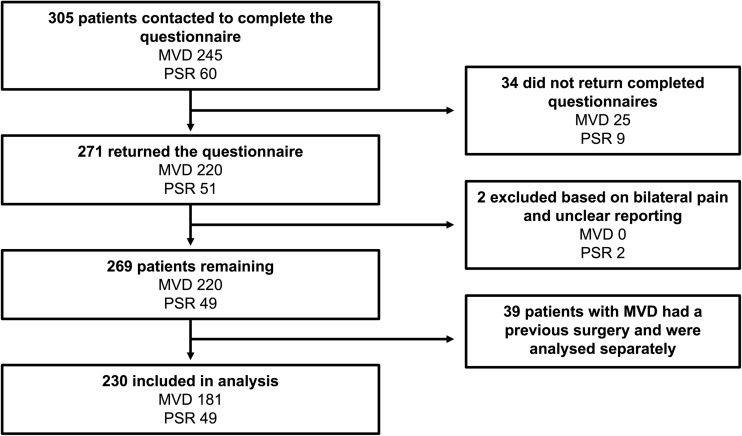
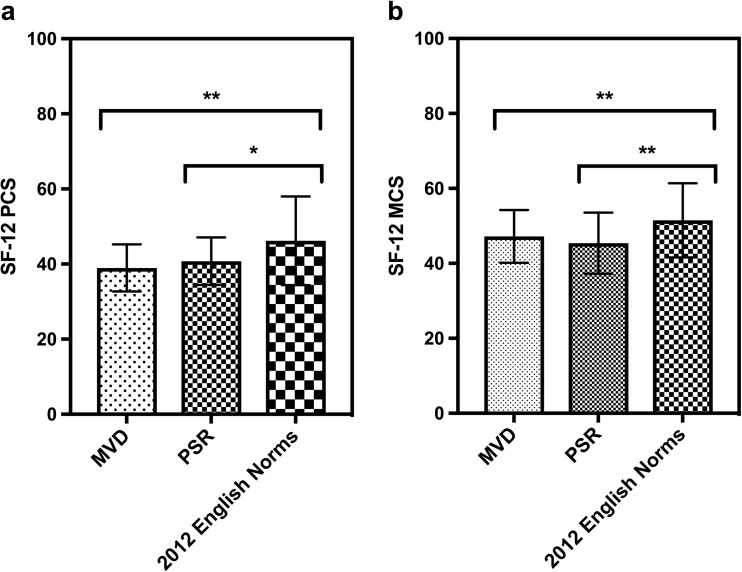
Results: One hundred and eighty-one of 245 (73.9%) patients after first MVD and 49 of 60 (81.7%) after PSR responded, and were included in analyses. The mean SF-12 scores of patients after MVD and PSR at five-year follow-up were significantly lower than English age-matched norms. Though there were no differences in SF-12 physical or mental component scores between the two procedures, patients after PSR were more likely to have case-level anxiety (RR = 3.3; 95% CI, 1.1-10.5; p = 0.03), had more postoperative complications, and of greater severity, including pain (RR = 2.52; 95% CI, 1.5-4.1; p < 0.001), numbness (RR = 5.9; 95% CI, 3.8-9.2; p < 0.001), burning sensations (RR = 3.0; 95% CI, 1.5-5.8; p = 0.001) and difficulty in eating (RR = 17.1; 95% CI, 5.6-53.1; p < 0.001), and these had a larger impact on quality of life for PSR compared to MVD.
Conclusions: The quality of life 5 years after MVD or PSR is poorer than in the general population and associated with postoperative complications such as pain, numbness, burning sensation and difficulty in eating. These complications are commoner after PSR than MVD, and this is associated with anxiety in PSR patients at five-year follow-up. However, these differences are not reflected by quality of life scores. Outcome measures need to incorporate patient experience after treatment for TN, and represent patient priorities for quality of life.
Keywords: PROMs; Posterior fossa surgery; Trigeminal neuralgia.
Conflict of interest statement
Conflict of interest
The authors have no known conflicts of interest to declare. All authors contributed to the design of the study. J.Z. designed and distributed the assessment set and organised its data entry. A.W. converted all the data into SPSS, and assisted with interpretation of psychometric data. D.J. analysed the data and wrote the first draft. All authors contributed equally to the subsequent revision and acceptance of the final manuscript, and are accountable for all aspects of the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional committee and with the latest amendment of the Helsinki declaration.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
Similar articles
-
Efficacy and safety of microvascular decompression with or without partial sensory rhizotomy: a comprehensive meta-analysis and systematic review in treating trigeminal neuralgia.Neurosurg Rev. 2024 May 24;47(1):229. doi: 10.1007/s10143-024-02463-4. Neurosurg Rev. 2024. PMID: 38787487
-
Efficacy and Prognostic Value of Partial Sensory Rhizotomy and Microvascular Decompression for Primary Trigeminal Neuralgia: A Comparative Study.Med Sci Monit. 2017 May 15;23:2284-2291. doi: 10.12659/msm.901510. Med Sci Monit. 2017. PMID: 28502974 Free PMC article.
-
Long-term efficacy and safety of internal neurolysis for trigeminal neuralgia without neurovascular compression.J Neurosurg. 2015 May;122(5):1048-57. doi: 10.3171/2014.12.JNS14469. Epub 2015 Feb 13. J Neurosurg. 2015. PMID: 25679283
-
Patient reports of satisfaction after microvascular decompression and partial sensory rhizotomy for trigeminal neuralgia.Neurosurgery. 2005 Jun;56(6):1304-11; discussion 1311-2. doi: 10.1227/01.neu.0000159883.35957.e0. Neurosurgery. 2005. PMID: 15918947 Clinical Trial.
-
First treatment and retreatment of medically refractive trigeminal neuralgia by stereotactic radiosurgery versus microvascular decompression: a systematic review and Meta-analysis.Br J Neurosurg. 2018 Aug;32(4):355-364. doi: 10.1080/02688697.2018.1472213. Epub 2018 May 10. Br J Neurosurg. 2018. PMID: 29745268
Cited by
-
Nerve Compression Syndromes in the Posterior Cranial Fossa.Dtsch Arztebl Int. 2019 Jan 25;116(4):54-60. doi: 10.3238/arztebl.2019.0054. Dtsch Arztebl Int. 2019. PMID: 30855007 Free PMC article. Review.
-
Treatment of redo-microvascular decompression or internal neurolysis plus microvascular decompression for recurrent trigeminal neuralgia: a review of long-term effectiveness and safety.J Int Med Res. 2022 Mar;50(3):3000605221080721. doi: 10.1177/03000605221080721. J Int Med Res. 2022. PMID: 35249412 Free PMC article. Review.
-
Psychological assessment in patients affected by trigeminal neuralgia. A systematic review.Neurosurg Rev. 2025 May 13;48(1):414. doi: 10.1007/s10143-025-03556-4. Neurosurg Rev. 2025. PMID: 40355578 Free PMC article. Review.
-
Efficacy and safety of CT-guided percutaneous pulsed radiofrequency treatment of the Gasserian ganglion in patients with medically intractable idiopathic trigeminal neuralgia.J Pain Res. 2018 Nov 19;11:2877-2885. doi: 10.2147/JPR.S179228. eCollection 2018. J Pain Res. 2018. PMID: 30510444 Free PMC article.
-
Altered Structural and Functional Abnormalities of Hippocampus in Classical Trigeminal Neuralgia: A Combination of DTI and fMRI Study.J Healthc Eng. 2022 Nov 30;2022:8538700. doi: 10.1155/2022/8538700. eCollection 2022. J Healthc Eng. 2022. PMID: 36504636 Free PMC article.
References
-
- Gronseth G, Cruccu G, Alksne J, Argoff C, Brainin M, Burchiel K, Nurmikko T, Zakrzewska JM. Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology. 2008;71:1183–1190. doi: 10.1212/01.wnl.0000326598.83183.04. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
