

Height and body fatness and colorectal cancer risk: an update of the WCRF-AICR systematic review of published prospective studies
- PMID: 29080978
- PMCID: PMC6060816
- DOI: 10.1007/s00394-017-1557-1
Height and body fatness and colorectal cancer risk: an update of the WCRF-AICR systematic review of published prospective studies
Abstract
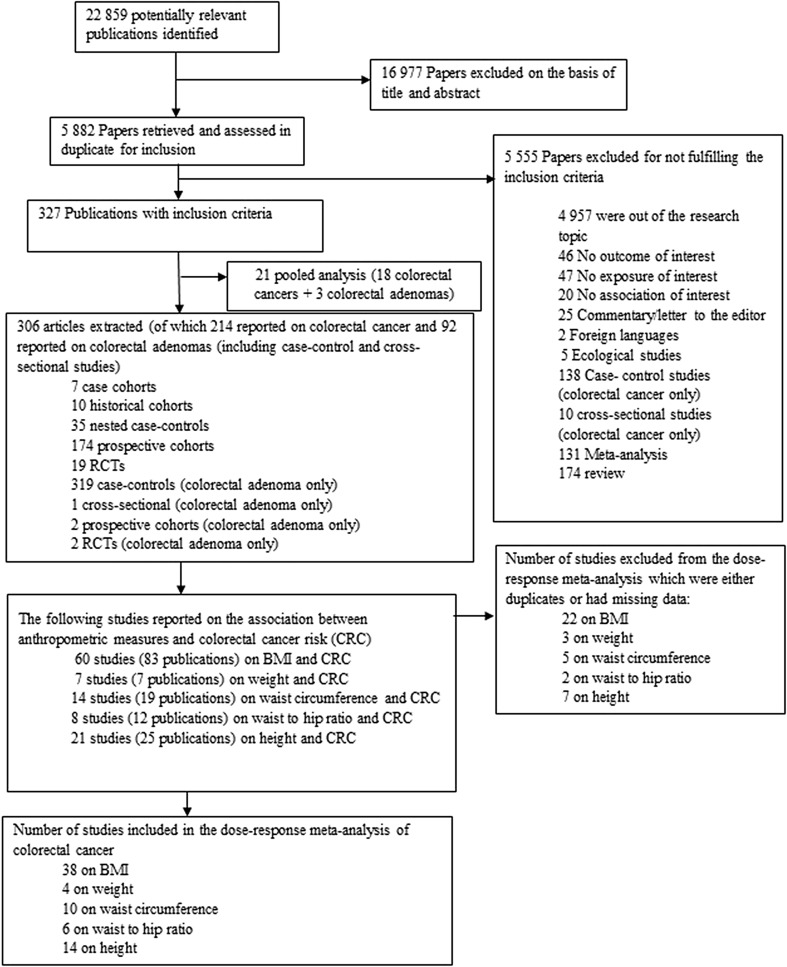
Purpose: There is no published dose-response meta-analysis on the association between height and colorectal cancer risk (CRC) by sex and anatomical sub-site. We conducted a meta-analysis of prospective studies on the association between height and CRC risk with subgroup analysis and updated evidence on the association between body fatness and CRC risk.
Methods: PubMed and several other databases were searched up to November 2016. A random effects model was used to calculate dose-response summary relative risks (RR's).
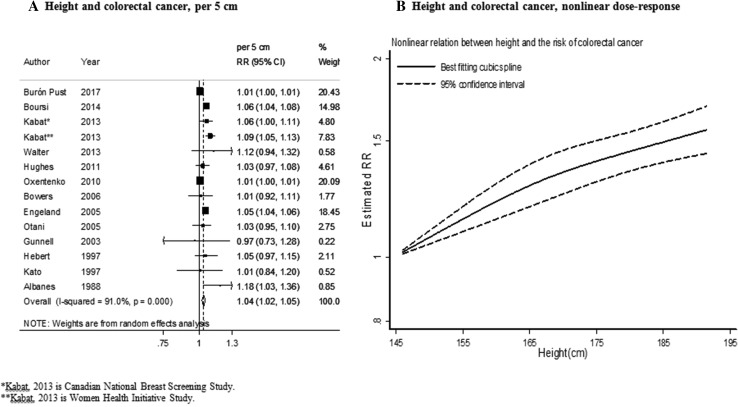
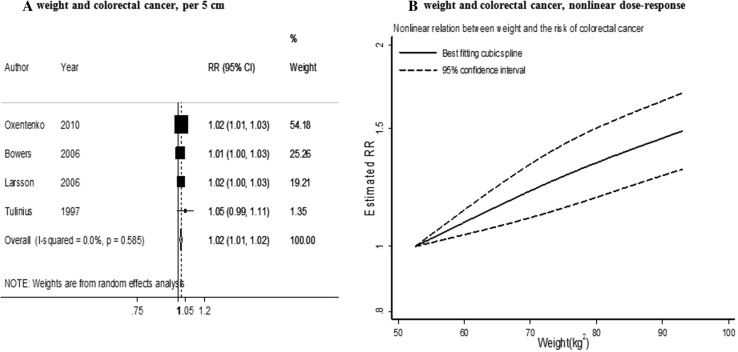
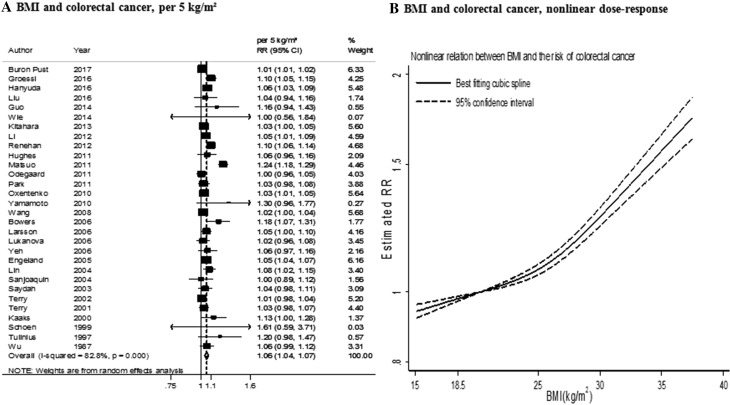
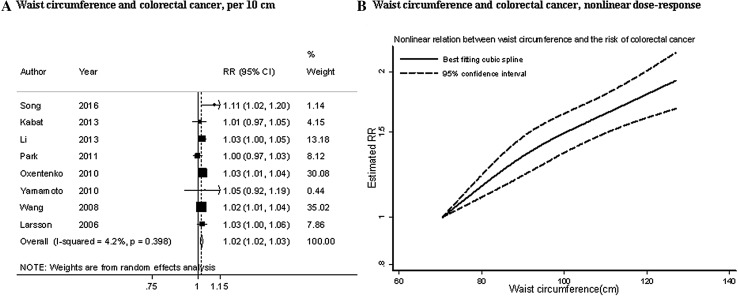
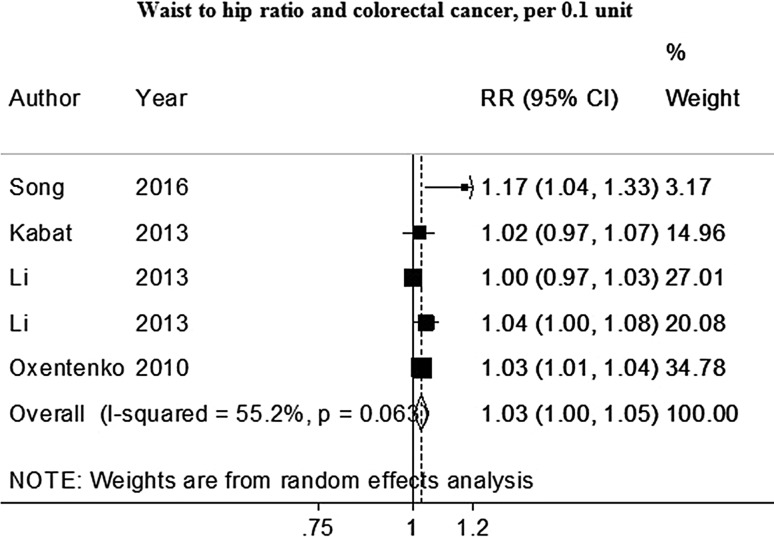
Results: 47 studies were included in the meta-analyses including 50,936 cases among 7,393,510 participants. The findings support the existing evidence regarding a positive association of height, general and abdominal body fatness and CRC risk. The summary RR were 1.04 [95% (CI)1.02-1.05, I² = 91%] per 5 cm increase in height, 1.02 [95% (CI)1.01-1.02, I² = 0%] per 5 kg increase in weight, 1.06 [95% (CI)1.04-1.07, I² = 83%] per 5 kg/m2 increase in BMI, 1.02 [95% (CI)1.02-1.03, I² = 4%] per 10 cm increase in waist circumference, 1.03 [95% (CI)1.01-1.05, I² = 16%] per 0.1 unit increase in waist to hip ratio. The significant association for height and CRC risk was similar in men and women. The significant association for BMI and CRC risk was stronger in men than in women.
Conclusion: The positive association between height and risk of CRC suggests that life factors during childhood and early adulthood might play a role in CRC aetiology. Higher general and abdominal body fatness during adulthood are risk factors of CRC and these associations are stronger in men than in women.
Keywords: BMI; Colorectal cancer; Continuous update project; Height; Meta-analysis.
Conflict of interest statement
Funding
This work was funded by the World Cancer Research Fund network (grant number 2007/SP01) as part of the Continuous Update Project. The work of SS and DA was supported by a NHS BRC grant (Interventional Public Health).
Conflict of interest
None of the authors reported a conflict of interest related to the study.
Figures
References
-
- World Cancer Research Fund/American Institute forCancer Research . Food, nutrition, physical activity, and the prevention of colorectal cancer. Washington, DC: AICR; 2011.
Ref Type: Online Source
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
