

Glioblastoma Treatment in the Elderly
- PMID: 29081442
- PMCID: PMC5735230
- DOI: 10.2176/nmc.ra.2017-0009
Glioblastoma Treatment in the Elderly
Abstract
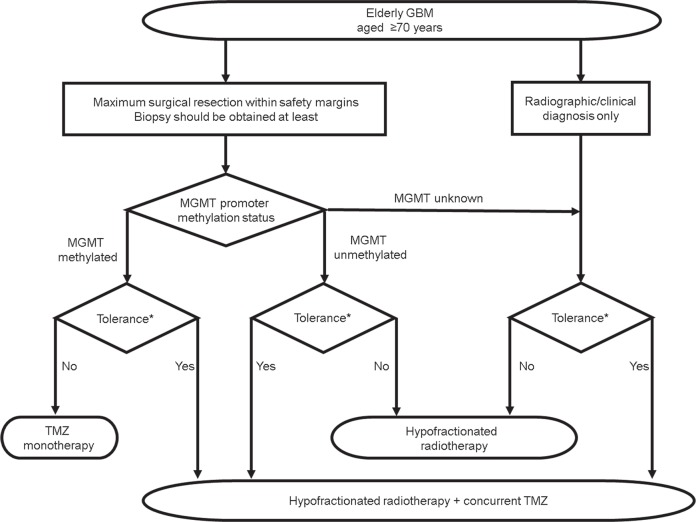
Although current treatment advances prolong patient survival, treatment for glioblastoma (GBM) in the elderly has become an emerging issue. The definition of "elderly" differs across articles; GBM predominantly occurs at an age ≥65 years, and the prognosis worsens with increasing age. Regarding molecular markers, isocitrate dehydrogenase (IDH) mutations are less common in the elderly with GBM. Meanwhile, O6-methylguanine DNA methyltransferase (MGMT) promoter methylation has been identified in approximately half of patients with GBM. Surgery should be considered as the first-line treatment even for elderly patients, and maximum safe resection is recommended if feasible. Concurrently, radiotherapy is the standard adjuvant therapy. Hypofractionated radiotherapy (e.g., 40 Gy/15 Fr) is suitable for elderly patients. Studies also supported the concurrent use of temozolomide (TMZ) with radiotherapy. In cases wherein elderly patients cannot tolerate chemoradiation, TMZ monotherapy is an effective option when MGMT promoter methylation is verified. Conversely, tumors with MGMT unmethylated promoter may be treated with radiotherapy alone to reduce the possible toxicity of TMZ. Meanwhile, the efficacy of bevacizumab (BEV) in elderly patients remains unclear. Similarly, further studies on the efficacy of carmustine wafers are needed. Based on current knowledge, we propose a treatment diagram for GBM in the elderly.
Keywords: elderly; glioblastoma; review; treatment.
Conflict of interest statement
All authors completed a self-declaration of the conflicts of interest (COI) to the Japan Neurosurgical Society and declare no potential COI regarding this manuscript.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group : Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352: 987–996, 2005 - PubMed
-
- Committee of Brain Tumor Registry of Japan : Report of the Brain Tumor Registry of Japan (2001–2004). Neurol Med Chir (Tokyo) 54: 1–102, 2014
-
- Gulati S, Jakola AS, Johannesen TB, Solheim O: Survival and treatment patterns of glioblastoma in the elderly: a population-based study. World Neurosurg 78: 518–526, 2012 - PubMed
-
- Zinn PO, Colen RR, Kasper EM, Burkhardt JK: Extent of resection and radiotherapy in GBM: A 1973 to 2007 surveillance, epidemiology and end results analysis of 21,783 patients. Int J Oncol 42: 929–934, 2013 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials