

Arthroscopic Lateral Ligament Repair Through Two Portals in Chronic Ankle Instability
- PMID: 29081860
- PMCID: PMC5633705
- DOI: 10.2174/1874325001711010617
Arthroscopic Lateral Ligament Repair Through Two Portals in Chronic Ankle Instability
Abstract
Objectives: Injury to the lateral ligament complex of the ankle is one of the most common sports-related injury. Usually lateral ankle evolves with excellent clinical recovery with non surgical treatment, however, near about 30% develop a lateral chronic instability sequela. Several open and arthroscopic surgical techniques have been described to treat this medical condition.
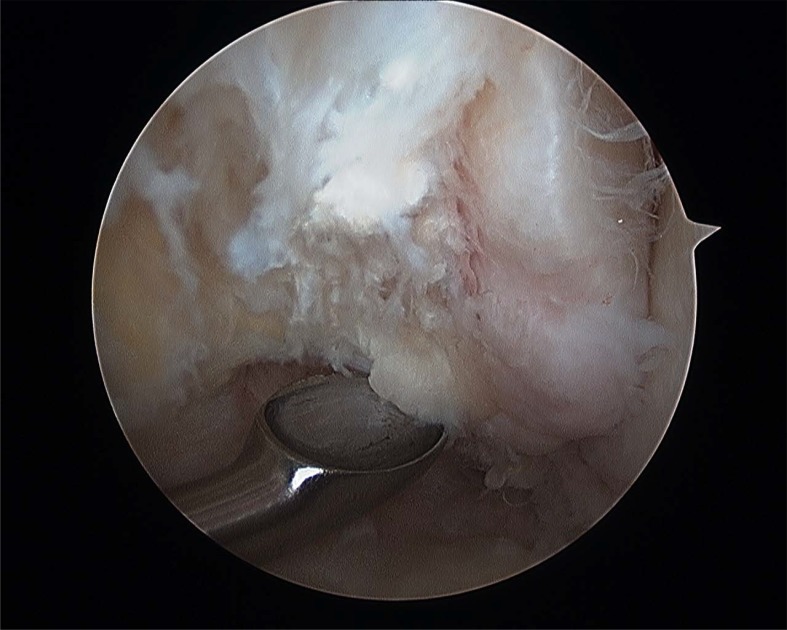
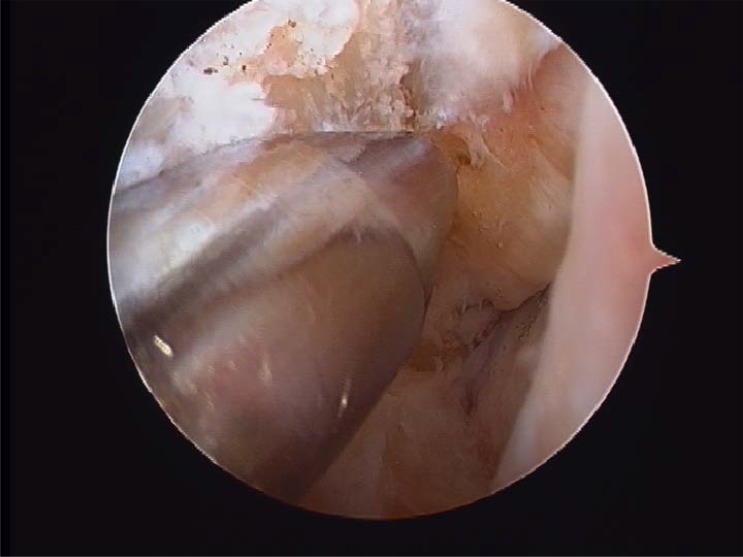
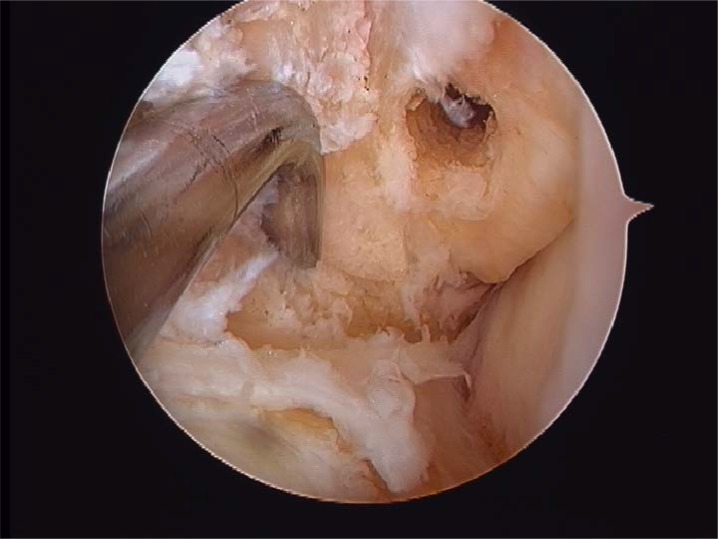
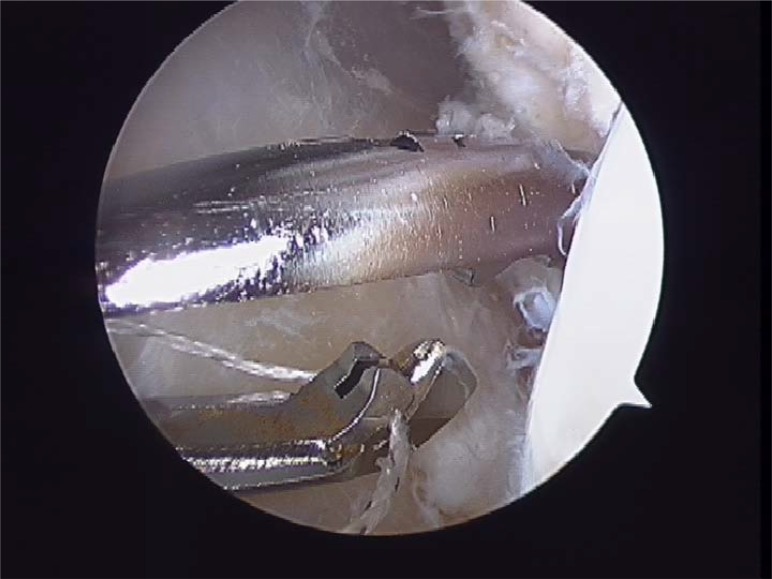
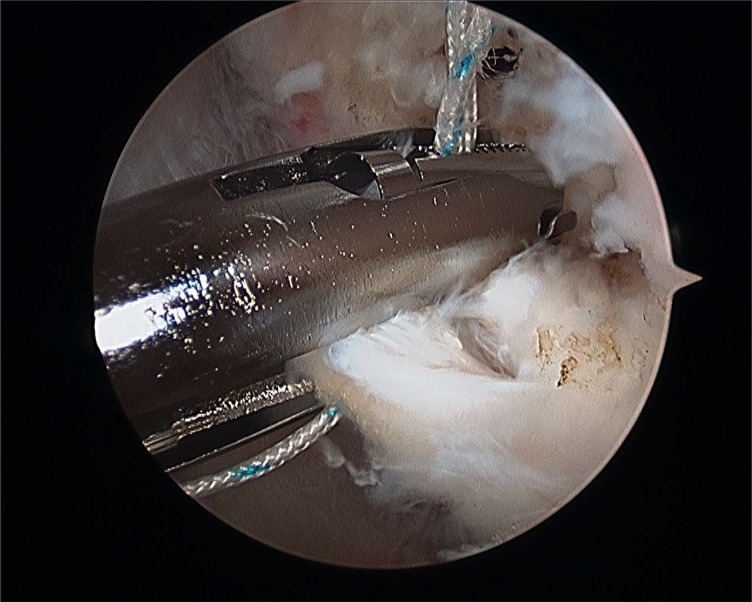
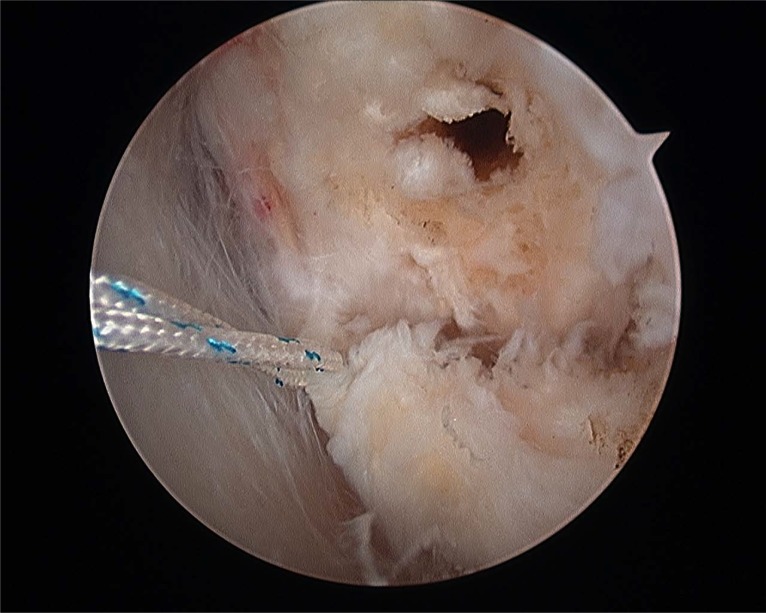
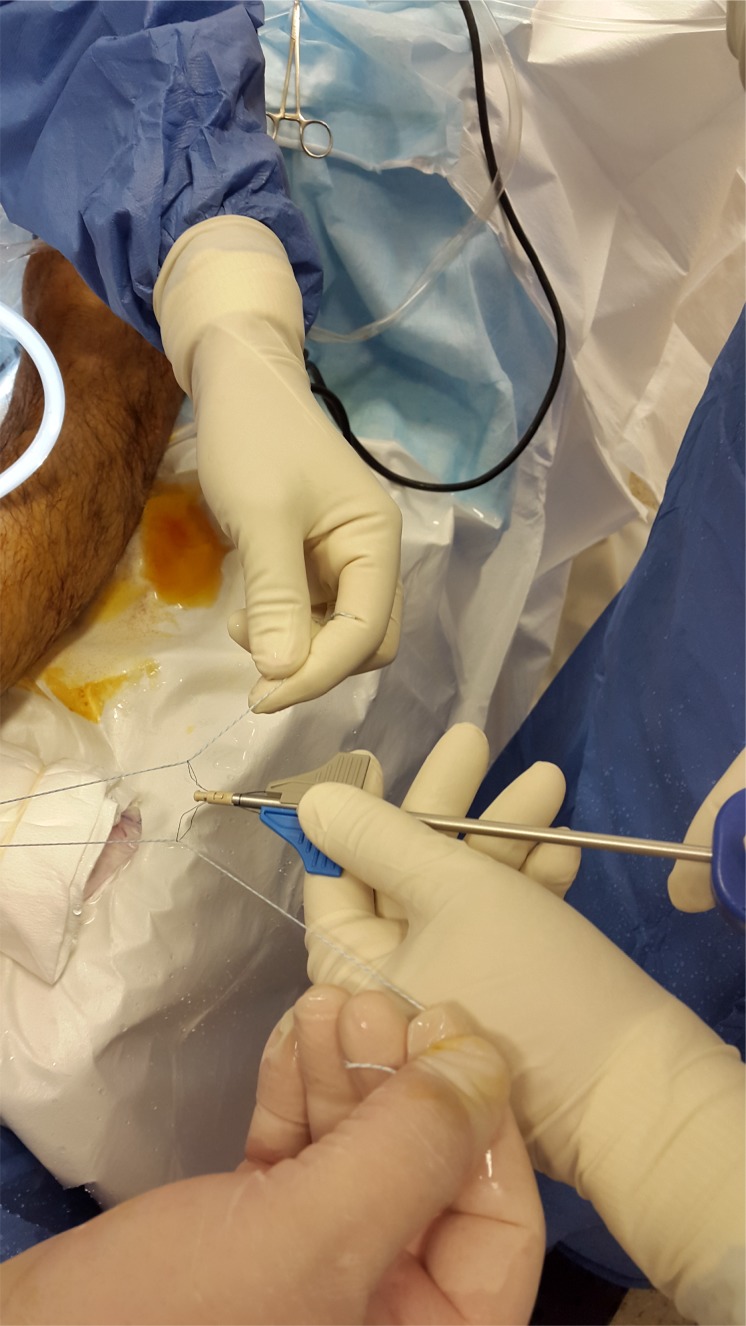
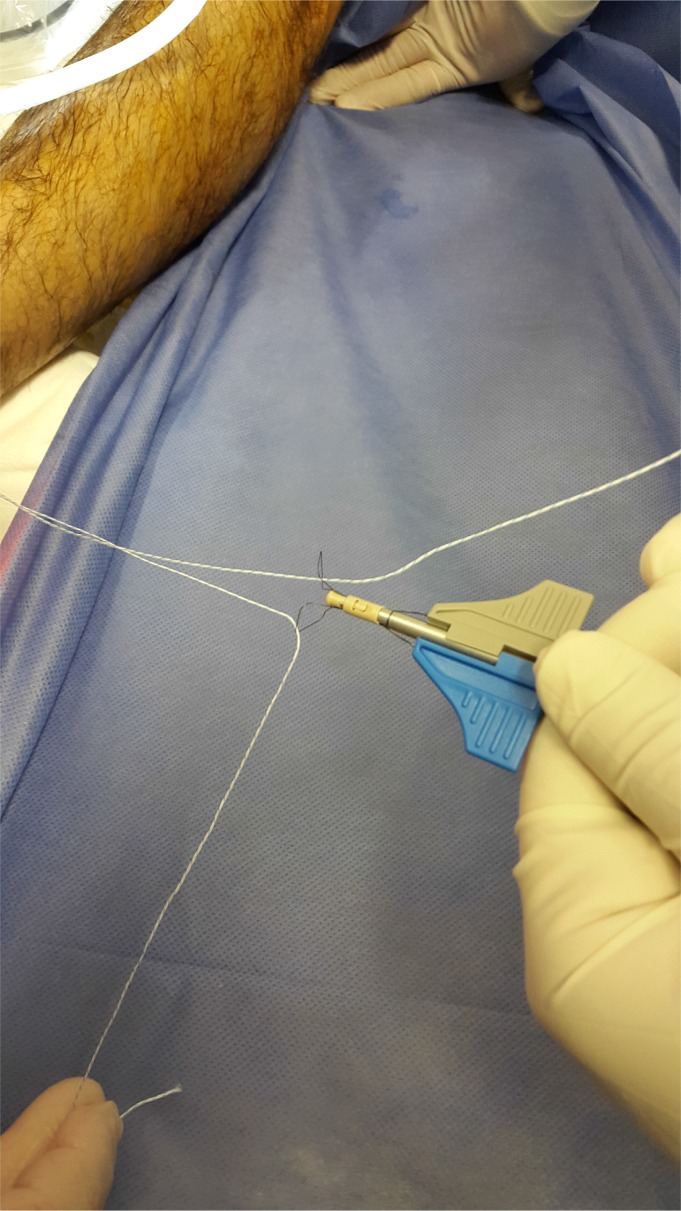
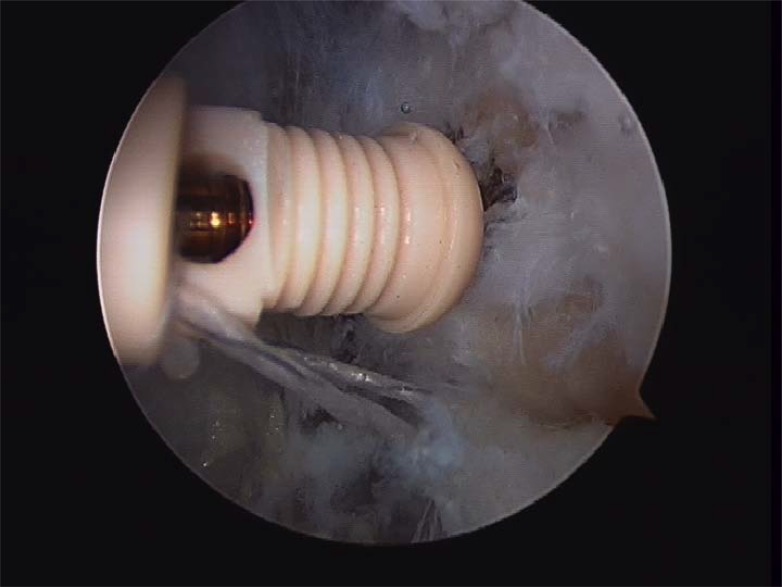
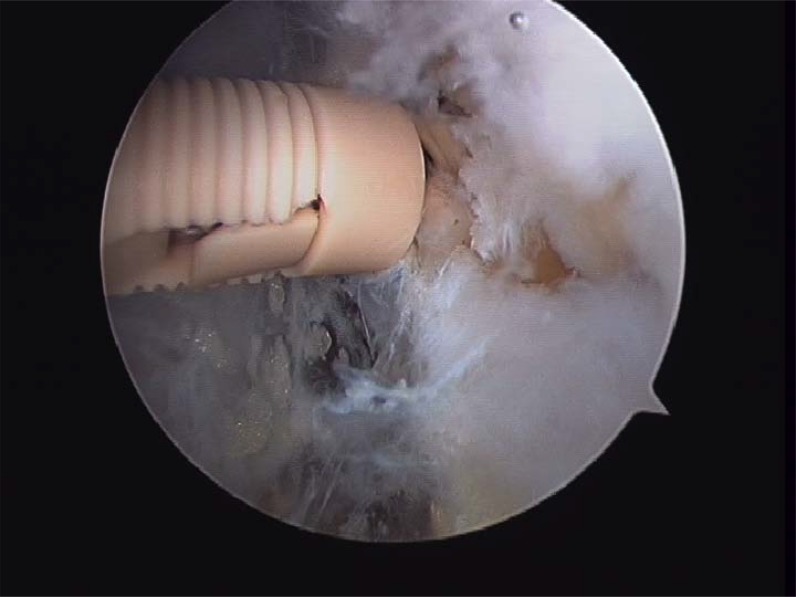
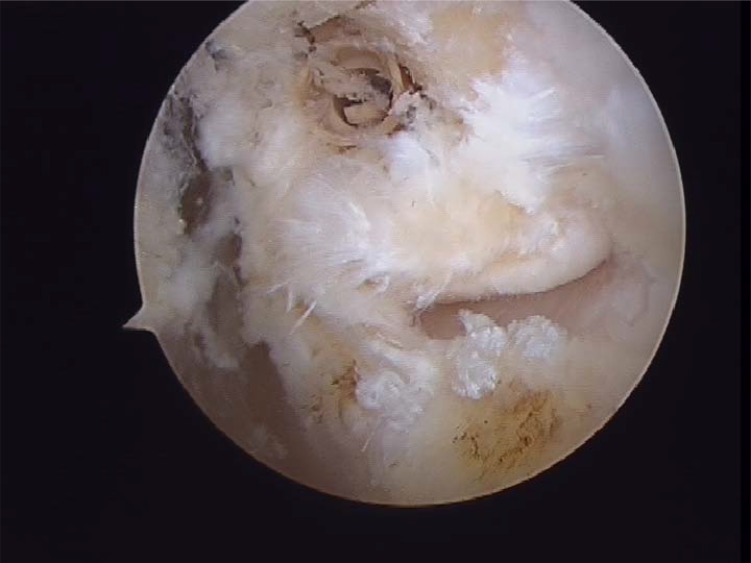
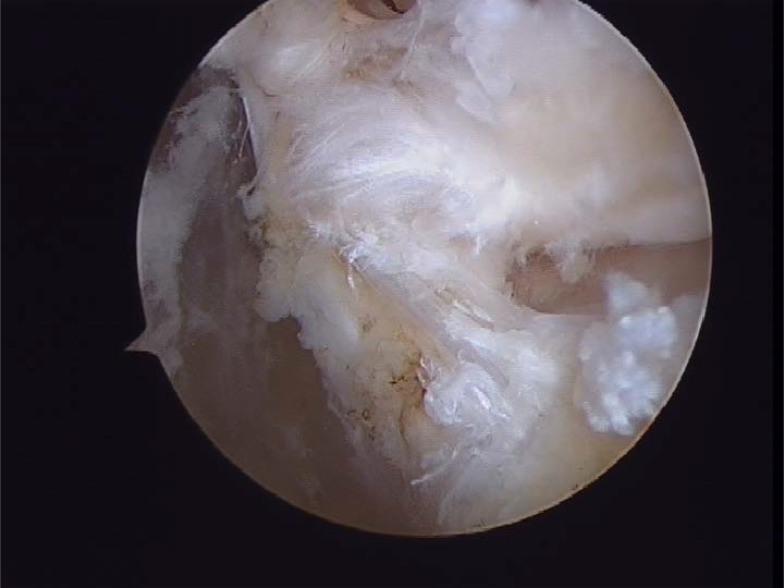
Material and methods: Of the 22 patients who were treated; 18 males and 4 females, and aged from 17-42 years (mean 28 years). All patients presented a history of more than three ankle sprains in the last two years and presented positive anterior drawer and talar tilt test of the ankle in the physical examination. We perform an anterior arthroscopy of the ankle in order to treat asociated disease and then we performed "All inside¨ lateral ligament repair through two portals (anteromedial and anterolateral) using an anchor knotless suture.
Results: Clinical outcome evaluations were performed at a mean follow up of 25 months. (R: 17-31). Overall results has been shown by means of the American Orthopaedic Foot and Ankle Society (AOFAS). Mean AOFAS scores improved from 63 points (range 52-77) preoperatively to 90 points (range 73-100) at final follow up. No recurrences of ankle instability were found in the cases presented.
Conclusion: Several surgical procedures have been described during the last years in order to treat chronic ankle instability. ¨All inside¨ lateral ligament reconstruction presents lower local morbidity than open procedures with few complications. Moreover, it is a reproductible technique, with high clinical success rate, few complications and relatively quick return to sports activities. A high knowledge of the anatomic landmarks should be essential to avoid unwated injuries.
Keywords: Ankle; Arthroscopy; Chronic instability; Reconstruction.
Figures








References
-
- Freeman M.A. Instability of the foot after injuries to the lateral ligament of the ankle. J. Bone Joint Surg. Br. 1965;47(4):669–677. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources