

Schistosomiasis-A Disobedient Ureter, a Disobedient Diagnosis
- PMID: 29082328
- PMCID: PMC5628567
- DOI: 10.1089/cren.2017.0042
Schistosomiasis-A Disobedient Ureter, a Disobedient Diagnosis
Abstract
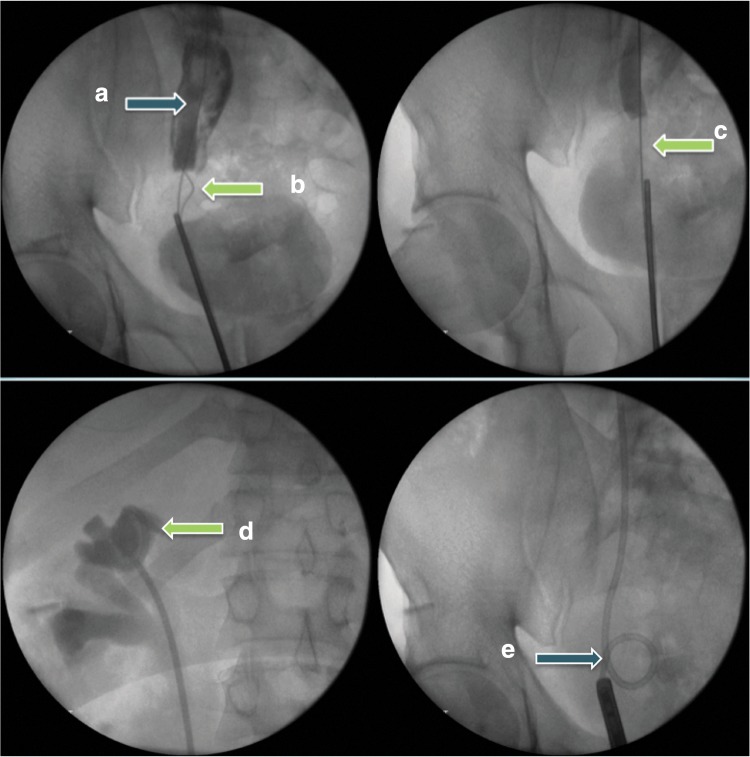
Background: Schistosomiasis is rare in western countries, but remains a potentially serious disease. It is known to result in severe urogenital complications; prompt diagnosis can therefore significantly affect outcomes. Case Presentation: We report the case of a 41-year-old male with pleuritic chest pain and visible hematuria who had emigrated from Zimbabwe to the United Kingdom 20 years previously. CT imaging revealed a hydronephrotic right pelvicaliceal system, with a dilated ureter to its distal portion. Preliminary tests for schistosomiasis, including terminal urine microscopy and serology, were negative. An initial ureteroscopy was challenging owing to a tight ureteral stricture such that a retrograde stent insertion and not ureteroscopic visualization or biopsy was carried out. A relook ureteroscopy after 6 weeks revealed a dense distal ureteral stricture, biopsies were taken, the stricture was ablated with LASER, and a retrograde stent was placed. Microscopic examination of the biopsies confirmed Schistosomiasis haematobium. Treatment consisted of a divided dose of praziquantel and a reducing dose of steroids. At a third look ureteroscopy the stricture was ablated with LASER again, and the stent was removed. Subsequent renograms indicated recurrent obstruction despite LASER treatment and a retrograde ureteral stent was replaced. The patient ultimately had a Boari flap ureteral reimplant with good results. Conclusion: This case illustrates the clinical challenges of diagnosing and treating ureteral schistosomiasis. It shows that all the initial tests can be negative, but where the clinical picture points toward schistosomiasis it is worth persevering and a good tissue biopsy may be the only way to verify an otherwise elusive diagnosis.
Keywords: HIV; bilharzia; schistosomiasis; ureteral strictures; urogenital schistosomiasis.
Conflict of interest statement
No competing financial interests exist.
Figures



References
-
- Savioli L, Renganathan E, Montresor A, et al. Division of Control of Tropical Diseases, Schistomiasis and Intestinal Parasites Unit, World Health Organization. Control of schistosomiasis—A global picture. Parasitology Today 1997;13:444–448 - PubMed
-
- Bichler K, Savatovsky I, Naber K, et al. EAU Guidelines for the management of urogenital schistosomiasis. Eur Urol 2006;49:998–1003 - PubMed
-
- Coltart CE, Chew A, Storrar N, et al. Schistosomiasis presenting in travellers: A 15 year observational study at the Hospital for Tropical Diseases, London. Trans R Soc Trop Med Hyg 2015;109:214–220 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources