

Dose, Content, and Mediators of Family-Based Treatment for Childhood Obesity: A Multisite Randomized Clinical Trial
- PMID: 29084318
- PMCID: PMC6169780
- DOI: 10.1001/jamapediatrics.2017.2960
Dose, Content, and Mediators of Family-Based Treatment for Childhood Obesity: A Multisite Randomized Clinical Trial
Abstract
Importance: Elucidation of optimal dosing and treatment content is critical for health care providers, payers, and policy makers, as well as mechanisms of change to inform intervention delivery and training initiatives for childhood obesity.
Objectives: To evaluate effects, following a 4-month family-based behavioral weight loss treatment (FBT), of 2 doses (HIGH or LOW) of a weight-control intervention (enhanced social facilitation maintenance [SFM+]) vs a weight-control education condition (CONTROL; matched for dose with LOW), on child anthropometrics, and to explore putative mediators of weight loss outcomes.
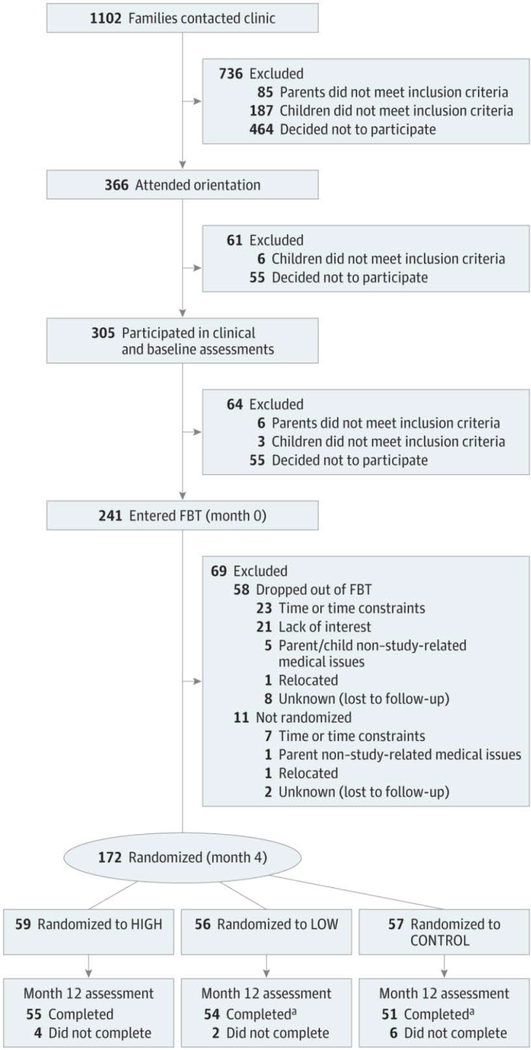
Design, setting, and participants: For this parallel-group randomized clinical trial conducted at 2 US academic medical centers from December 2009 to March 2013, 172 parent-child dyads completed FBT and were then randomized to 8 months of SFM+ (HIGH, n = 59; LOW, n = 56) or CONTROL (n = 57). Children (aged 7-11 years) with overweight and obesity (body mass index [BMI; calculated as weight in kilograms divided by height in meters squared] ≥85th percentile) with at least 1 parent with overweight and obesity (BMI ≥25) were recruited.
Interventions: HIGH SFM+ vs LOW SFM+ (CONTROL matched the dose of LOW).
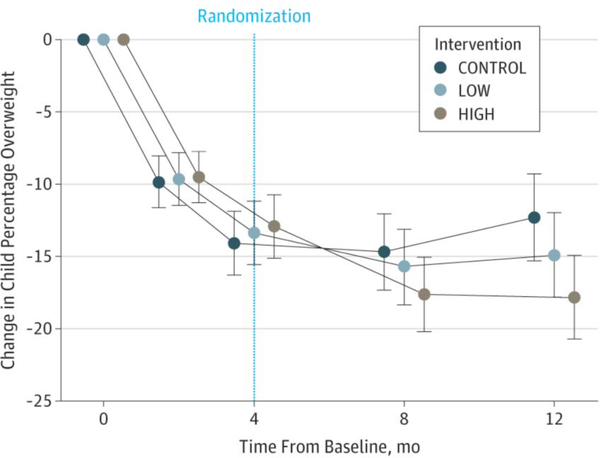
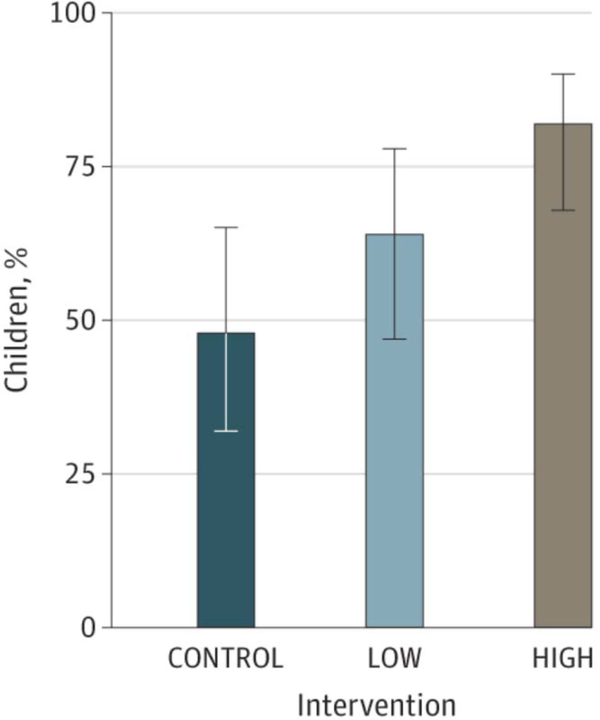
Main outcomes and measures: Intention-to-treat analysis using mixed-effects models estimated change in child percentage overweight (percentage above the median BMI for a child's age and sex) for the FBT period (0-4 months) and the SFM+ period (4-12 months), and proportion of children achieving a clinically significant change in percentage overweight (≥9-unit decrease; months 0-12). Theory-based outcome mediators were also evaluated.
Results: This study recruited 172 parent-child dyads (mean [SD] age: parents 42.3 [6.4] years; children, 9.4 [1.3] years). The omnibus treatment × time interaction for child percentage overweight was significant (F8, 618.9 = 2.89; P = .004). Planned pairwise comparisons revealed that from months 4 to 12, LOW had better outcomes than CONTROL (difference, -3.34; 95% CI, -6.21 to -0.47; d = -0.40; P = .02). HIGH had better outcomes than LOW (difference, -3.37; 95% CI, -6.15 to -0.59; d = -0.38; P = .02) and CONTROL (difference, -6.71; 95% CI, -9.57 to -3.84; d = -0.77; P < .001). A greater proportion of children in HIGH (45 [82%]) vs LOW (34 [64%]) (difference, 18.00; 95% CI, 1.00-34.00; P = .03; number needed to treat = 5.56) and CONTROL (25 [48%]) (difference, 34.00; 95% CI, 16.00-51.00; P < .001; number needed to treat = 2.94) had clinically significant percentage overweight reductions. Food and activity monitoring and goal setting mediated the effect of LOW vs CONTROL (50%). Monitoring and goal setting, family and home environment, and healthy behaviors with peers mediated the effect of HIGH vs CONTROL (25%-42%).
Conclusions and relevance: Following FBT, specialized intervention content (SFM+) enhanced children's weight outcomes and outperformed a credible control condition, with high dose delivery yielding the best outcomes. Sustained monitoring and goal setting, support from the family and home environment, and healthy peer interactions explained outcome differences, highlighting key treatment targets.
Trial registration: clinicaltrials.gov Identifier: NCT00759746.
Figures
References
-
- Halfon N, Larson K, Slusser W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad Pediatr. 2013;13(1):6–13. - PubMed
-
- Hampl SE, Carroll CA, Simon SD, Sharma V. Resource utilization and expenditures for overweight and obese children. Arch Pediatr Adolesc Med. 2007;161(1):11–14. - PubMed
-
- Preventive US Services Task Force. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. Pediatrics. 2010;125(2):361–367. - PubMed
-
- O’Connor EA, Evans CV, Burda BU, Walsh ES, Eder M, Lozano P. Screening for Obesity and Intervention for Weight Management in Children and Adolescents: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2017;317(23):2427–2444. - PubMed
-
- Whitlock EP, O’Connor EA, Williams SB, Beil TL, Lutz KW. Effectiveness of weight management interventions in children: a targeted systematic review for the USPSTF. Pediatrics. 2010;125(2):e396–418. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- T32 HL007456/HL/NHLBI NIH HHS/United States
- T32 MH018269/MH/NIMH NIH HHS/United States
- K24 MH070446/MH/NIMH NIH HHS/United States
- P30 DK056341/DK/NIDDK NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- R01 HD036904/HD/NICHD NIH HHS/United States
- UL1 RR025014/RR/NCRR NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- KL2 RR024994/RR/NCRR NIH HHS/United States
- UL1 TR000423/TR/NCATS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- K23 DK060476/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
