

Community-based psychosocial interventions for people with schizophrenia in low and middle-income countries: systematic review and meta-analysis
- PMID: 29084529
- PMCID: PMC5661919
- DOI: 10.1186/s12888-017-1516-7
Community-based psychosocial interventions for people with schizophrenia in low and middle-income countries: systematic review and meta-analysis
Abstract
Background: There is consensus that the treatment of schizophrenia should combine anti-psychotic medication and psychosocial interventions in order to address complex social, economic and health needs. It is recommended that family therapy or support; community-based rehabilitation; and/or self-help and support groups should be provided for people with schizophrenia in low and middle-income countries. The effectiveness of community-based psychosocial interventions in these settings is unclear.
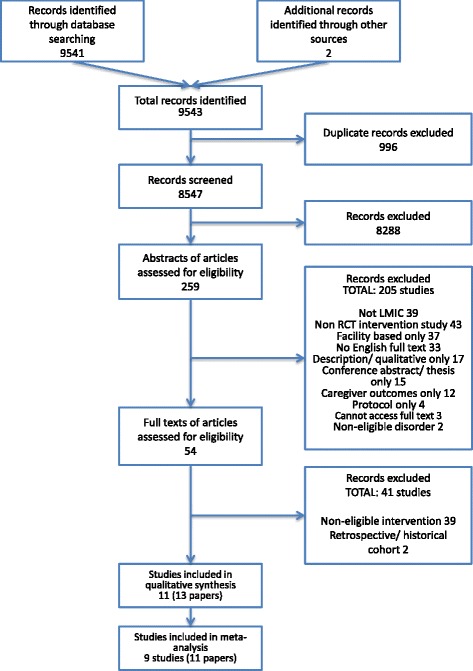
Methods: Studies evaluating community-based psychosocial interventions for people with schizophrenia were identified through database searching up to April 2016. Randomised controlled trials were included if they compared the intervention group with a control group receiving treatment as usual including medication. Only studies set in low and middle-income countries were included. Random effects meta-analyses were performed separately for each intervention type.
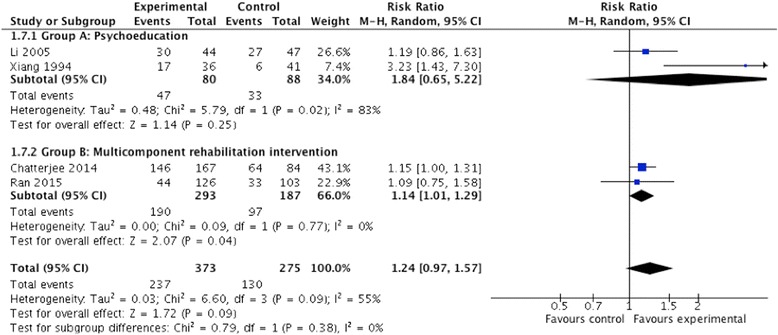
Results: Eleven randomised controlled trials in five middle-income countries were identified, with a total of 1580 participants. The content of included interventions varied from single-faceted psychoeducational interventions, to multi-component rehabilitation-focused interventions, to case management interventions. A third of the included studies did not incorporate any community involvement in the intervention. The quality of evidence was often low. Amongst the seven studies that reported on symptom severity up to 18 months post intervention, the pooled standardised mean difference (SMD) across all intervention types was 0.95 (95% CI 0.28, 1.61; P 0.005; I 2 = 95%; n = 862), representing a strong effect. A strong effect on symptom severity remained after excluding two studies with a high risk of bias (SMD 0.80; 95% CI 0.07, 1.53; P 0.03; I 2 = 94%; n = 676). Community-based psychosocial interventions may also have beneficial impacts on functioning (SMD 1.12; 95% CI 0.25, 2.00; P 0.01; I 2 = 94%; n = 511) and reducing hospital readmissions (SMD 0.68; 95% CI 0.27, 1.09; P 0.001; I2 = 33%; n = 167).
Conclusion: The limited evidence from low and middle-income countries supports the feasibility and effectiveness of community-based psychosocial interventions for schizophrenia, even in the absence of community mobilisation. Community-based psychosocial interventions should therefore be provided in these settings as an adjuvant service in addition to facility-based care for people with schizophrenia.
Keywords: Community mental health services; Disability; Low and middle-income countries; Psychiatric rehabilitation; Psychosis; Schizophrenia.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Patel V, Chisholm D, Parikh R, Charlson FJ, Degenhardt L, Dua T, Ferrari AJ, Hyman S, Laxminarayan R, Levin C, et al. Addressing the burden of mental, neurological, and substance use disorders: key messages from disease control priorities, 3rd edition. Lancet. 2015;387(10028):1672–1685. doi: 10.1016/S0140-6736(15)00390-6. - DOI - PubMed
-
- WHO . Psychosocial rehabilitation; a consensus statement. Geneva: World Health Organisation Division of Mental Health; 1996.
-
- Leucht S, Tardy M, Komossa K, Heres S, Kissling W, Davis JM. Maintenance treatment with antipsychotic drugs for schizophrenia. Cochrane Database Syst Rev. 2012;5:Cd008016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
