

Management of pregnancy at and beyond 41 completed weeks of gestation in low-risk women: a secondary analysis of two WHO multi-country surveys on maternal and newborn health
- PMID: 29084551
- PMCID: PMC5663145
- DOI: 10.1186/s12978-017-0394-2
Management of pregnancy at and beyond 41 completed weeks of gestation in low-risk women: a secondary analysis of two WHO multi-country surveys on maternal and newborn health
Abstract
Background: The World Health Organization (WHO) recommends induction of labour (IOL) for women who have reached 41 completed weeks of pregnancy without spontaneous onset of labour. Many women with prolonged pregnancy and/or their clinicians elect not to induce, and chose either elective caesarean section (ECS) or expectant management (EM). This study intended to assess pregnancy outcomes of IOL, ECS and EM at and beyond 41 completed weeks.
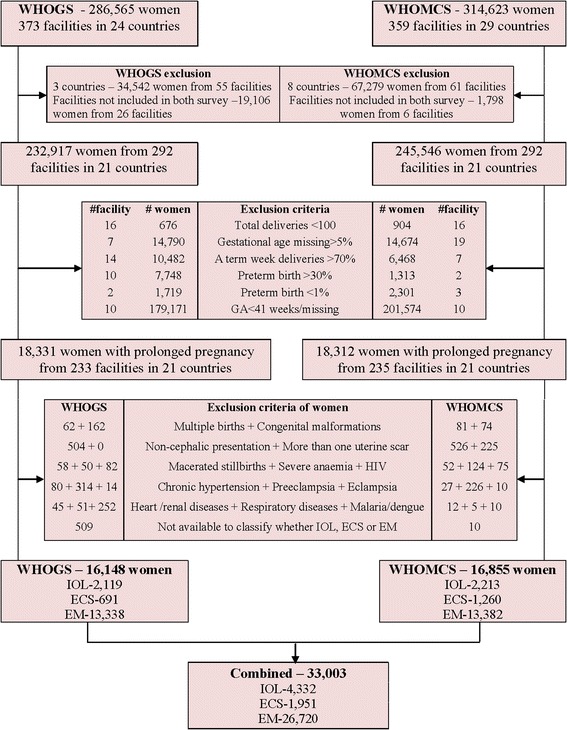
Methods: This study is a secondary analysis of the WHO Global Survey (WHOGS) and the WHO Multi-country Survey (WHOMCS) conducted in Africa, Asia, Latin America and the Middle East. There were 33,003 women with low risk singleton pregnancies at ≥41 completed weeks from 292 facilities in 21 countries. Multilevel logistic regression model was used to assess associations of different management groups with each pregnancy outcome accounted for hierarchical survey design. The results were presented by adjusted odds ratios (aORs) with 95% confidence intervals (CIs) after adjusting for age, education, marital status, parity, previous caesarean section (CS), birth weight, and facility capacity index score.
Results: The prevalence of prolonged pregnancy at facility setting in WHOGS, WHOMCS and combined databases were 7.9%, 7.5% and 7.7% respectively. Regarding to maternal adverse outcomes, EM was significantly associated with decreased risk of CS rate consistently in both databases i.e. (aOR0.76; 95% CI: 0.66-0.87) in WHOGS, (aOR0.67; 95% CI: 0.59-0.76) in WHOMCS and (aOR0.70; 95% CI: 0.64-0.77) in combined database, compared to IOL. Regarding the adverse perinatal outcomes, ECS was significantly associated with increased risks of neonatal intensive care unit admission (aOR1.76; 95% CI: 1.28-2.42) in WHOMCS and (aOR1.51; 95% CI: 1.19-1.92) in combined database compared to IOL but not significant in WHOGS database.
Conclusions: Compared to IOL, ECS significantly increased risk of NICU admission while EM was significantly associated with decreased risk of CS. ECS should not be recommended for women at 41 completed weeks of pregnancy. However, the choice between IOL and EM should be cautiously considered since the available evidences are still quite limited.
Keywords: Elective caesarean section; Expectant management; Induction of labour; Post-term pregnancy; Pregnancy outcomes; Prolonged pregnancy.
Conflict of interest statement
Ethics approval and consent to participate
The WHOGS and WHOMCS were approved by the WHO Ethical Review Committee and the relevant ethical clearance bodies in participating countries and facilities. Written consent from individual women was not needed because there was no contact between the data collectors (who extracted routine medical record data) and individual women, and all data was anonymized.
Consent for publication
Not applicable.
Competing interests
The authors declared that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO. World Health Organization recommendations for induction of Labour 2011. http://apps.who.int//iris/handle/10665/44531. Accessed 24 Aug 2014.
-
- Martin JA, Hamilton BE, Ventura SJ. Et al.National Vital Statistics Reports. Report no. 1.Hyattsville, Maryland. United States of America: National Vital Statistics System; 2012.
-
- The Health and Social Care Information Centre.NHS Maternity Statistics 2011-2012 Summary report. Geneva, Switzerland: National Health Service; 2012. http://www.hscic.gov.uk/hes.
-
- Li Z,Zeki R, Hilder L, et al.Australian institute of health and welfare. Australia’s mothers and babies 2010.Canberra,ACT,Australia:AustralianInstitute ofHealth and welfare; 2012. http://www.aihw.gov.au/publication-detail/?id=60129542376.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
