

Effectiveness of sitagliptin compared to sulfonylureas for type 2 diabetes mellitus inadequately controlled on metformin: a systematic review and meta-analysis
- PMID: 29084794
- PMCID: PMC5665259
- DOI: 10.1136/bmjopen-2017-017260
Effectiveness of sitagliptin compared to sulfonylureas for type 2 diabetes mellitus inadequately controlled on metformin: a systematic review and meta-analysis
Abstract
Objective: To assess the effectiveness of sitagliptin compared to sulfonylureas as add-on to metformin in adults with type 2 diabetes mellitus from both randomised controlled trials (RCTs) and 'real-world' non-randomised studies.
Methods and analyses: We conducted a systematic review of EMBASE, MEDLINE, CENTRAL and grey literature for RCTs and non-randomised studies. We reported outcomes relating to change in HbA1c, fasting glucose, weight, blood pressure and lipids from baseline and need for treatment change. No study investigating macrovascular and microvascular diabetes complications was found. Meta-analysis was used where studies were sufficiently homogenous.
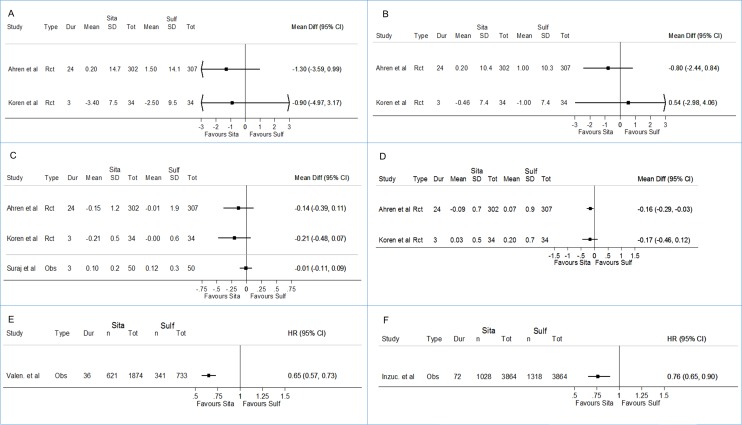
Results: Seven RCTs and five non-randomised studies were eligible for inclusion from 1335 articles retrieved. Meta-analysis of three homogenous RCTs revealed a statistically significant decrease in weight with sitagliptin when compared to sulfonylureas (weighted mean difference (WMD) -2.05 kg; 95% CI -2.38 to -1.71); however, a similar change from baseline in HbA1c (WMD 0.05; 95% CI -0.03 to 0.12), fasting glucose (WMD 0.11; 95% CI -0.08 to -0.29), blood pressure, lipids and the proportion achieving HbA1c <7% by study end (OR 0.98; 95% CI 0.85 to 1.13) was observed.Non-randomised studies identified consisted of four prospective and one retrospective cohort study. Three of these five studies were of moderate/high quality, and results though less precise suggested similar real-world comparative glycaemic and weight effectiveness for both treatments. Data from two cohort studies suggested that treatment change (HR 0.65; 95% CI 0.57 to 0.73) and insulin initiation (HR 0.76; 95% CI 0.65 to 0.90) were less likely among those prescribed sitagliptin; however, inadequate reporting of HbA1c at time of treatment change made interpreting results challenging.
Conclusion: Sitagliptin users experienced modest weight loss compared to gain with sulfonylureas; however, this difference was around 2 kg, which may not be of major clinical significance for most individuals. Similar change was observed across most other effectiveness outcomes reported. Further studies are needed to address longer-term effectiveness outcomes for sitagliptin compared to sulfonylureas as add-on to metformin.
Prospero registration number: CRD42016033983.
Keywords: meta-analysis; metformin; sitagliptin; sulfonylurea; systematic review; type 2 diabetes.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: All authors have completed the International Committee of Medical Journal Editors uniform disclosure form at www.icmje.org/coi_disclosure.pdf. MS, IN and IP report grants from Novo Nordisk A/S, during the conduct of the study. The authors (MS, NB, IN and IP) do not declare any conflicts of interest relevant to this manuscript.
Figures


References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the study of Diabetes. Diabetes Care 2015;38:140–9. 10.2337/dc14-2441 - DOI - PubMed
-
- National Institute of Clinical Excellence. NICE CG28: type 2 diabetes in adults: management. 2015. https://www.nice.org.uk/guidance/ng28/resources/type-2-diabetes-in-adult... (accessed 21 Jan 2016). - PubMed
-
- American Diabetes Association. Standards of medicare in diabetes: approaches to glycaemic treatment. Diabetes Care 2016;39:S52–9.
-
- International Diabetes Federation. IDF global guideline for type 2 diabetes. 2012. http://www.idf.org/guideline-type-2-diabetes (accessed 10 July 2016).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical